
June 3, 2019
By Jennifer S. Harthan, OD, FAAO, FSLS
Professor and Chief, Cornea Center for Clinical Excellence
Illinois College of Optometry
 Why try to control myopia progression?
Why try to control myopia progression?
Myopia has become increasingly widespread. As previously described, the prevalence of myopia has contributed to it becoming a ‘worldwide public health issue’.1-6 Reports have estimated that almost five billion individuals will suffer from myopia by the year 2050. 1,7 Due to this rampant escalation, practitioners have seen an influx of concern regarding myopia control. Contact lens manufacturers are enhancing lens designs and technologies, and there is an increasing number of educational resources available on the topics of myopia control and management.
Genetics, as well as visual behaviors contribute to myopia progression.8 The amount of time children spend outdoors8,9-14and time committed to near activities15 may also play a role. Myopia is associated with sight-threatening conditions such as cataracts, primary open angle glaucoma, retinal detachments, myopic maculopathy, and choroidal neovascular membranes.14,16-18 The higher the degree of myopia, the greater the risk of these conditions. Therefore, reducing an individual’s myopia progression also reduces the risk of these sight-threatening conditions.
What are the current treatments for controlling myopia?
There are two currently accepted treatments of myopia control: reducing the rate of myopia progression or delaying the onset of myopia.14 Several studies have established that previously accepted methods for myopia control such as under correction of myopia 14,19 single vision gas permeable contact lenses,14,20 and bifocal spectacles,14,21 may now be considered ineffective. The time that children spend outdoors may delay the onset of myopia, but not reduce the rate of myopia progression.11,12,14,22,23
The three most-researched treatment approaches that have validated a reduction in the long-term progression of myopia are orthokeratology, soft distance centered bifocal contact lenses,14,24-26, and antimuscarinic agents (atropine).14,27 Patients and parents must be educated that all treatments for myopia control are considered ‘off label’ as part of their informed consent process since there are currently no FDA approved products available with an indication for myopia control.
While all three of the treatments mentioned above are effective in controlling myopia progression, this brief review will focus only on overnight orthokeratology.
How does orthokeratology treat myopia progression?
Orthokeratology (ortho-k) refers to the use of gas permeable contact lenses, that are worn while asleep and removed upon awakening. They create a temporary change in shape of the cornea to correct for low- to-moderate amounts of myopia and astigmatism. Thus, glasses or contact lenses do not have to be worn during the day.1 While each lens design has its unique proprietary parameters, commonly shared features of commercially available ortho-k lenses include the following: a larger diameter, small treatment zone (optic zone), and a secondary or reverse curve steeper than the base curve.8 Ortho-k induces peripheral myopic defocus along the horizontal and vertical meridians.1,28-31 This increased myopic defocus along with reduced peripheral hyperopic blur leads to a decreased stimulus for eye growth, thus halting myopia progression.30
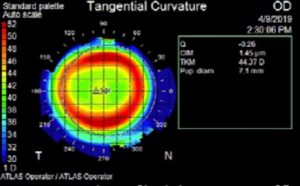
Figure 1: Tangential map following ortho-K lens wear for myopia control demonstrating proper centration and treatment. |

Ortho-k lens on the eye should provide the following: centration, adequate movement, and well-formed treatment, return, and alignment zones. |
What does the current literature say?
Concerned parents and practitioners alike often have several questions preceding ortho-k treatment. What is the most appropriate age to initiate ortho-k? When should ortho-k be initiated based on the amount and rate of myopia progression? Studies suggest that a young child between the ages of 6-9, who experience an increase in axial length of > 0.20mm/7 months and/or spherical equivalent of myopic progression of greater than or equal to one diopter per year, is an ideal candidate for ortho-k lenses.30,32
Ortho-k has been shown to reduce myopia progression by slowing axial length elongation by slightly less than 50%;14,33,34 ranging from 41-45% in most meta-analyses.1,35,36 When treating patients for myopia control with ortho-k, axial length measurements at baseline and throughout the treatment process are critical. Most studies routinely use axial length elongation as a measure for myopia progression rather than changes in spherical equivalent.30 Axial length elongation was found to be 0.23 + 0.25 mm in ortho-k lens wearers compared to 0.48 + 0.26 mm in single vision spectacle wearers in a two-year prospective pilot study on 35 children (ages 7-12 years).1,37 Throughout the duration of this study, ortho-k lens wearers had a 50% reduction in myopia progression.1,37 Additionally, a one-year study of anisometropic children 7-13 years of age found a statistically significant difference in axial length elongation between the ortho-k eye (0.07 + 0.21 mm, p= 0.038) and fellow eye with no correction (0.36 + 0.23 mm, p<0.001).30,38
In a five-year study of children (ages 8-12 years) fit with ortho-k lenses, myopia progression almost reduced by half during the first year of treatment as compared to children wearing single-vision spectacles.1,33 During the last three years of the study, there was no significant difference in myopia progression rates amongst the two groups. This possibly suggests a tapering effect of myopia control by ortho-k with longer periods of treatment.1,33
Future?
With the escalating incidence of myopia, we see advancements in lens designs and instruments. Manufacturers of orthokeratology lens designs are expanding parameters to correct for higher amounts of astigmatism and high myopia.1
While research on the subject matter of myopia control is broad and has answered many questions, further research is needed to comprehend this significant epidemic fully. No one treatment is 100% effective at slowing the rate of myopia progression. One thing is definite, it is imperative to optimize treatment plans for the individual patient, which may now include combination therapies. The overall goal is to ultimately prevent sight-threatening complications in these myopic individuals.

Jennifer S. Harthan OD, FAAO, FSLS, Professor and Chief, Cornea Center for Clinical Excellence, Illinois College of Optometry
References:
- Kang P. Optical and pharmacological strategies of myopia control. Clin Exp Optom 2018;101:321-32.
- Lin LL, Shih YF, Hsiao CK, Chen CJ. Prevalence of myopia in Taiwanese schoolchildren: 1983 to 2000. Ann Acad Med Singapore 2004;33:27-33.
- Vitale S, Sperduto RD, Ferris FL, 3rd. Increased prevalence of myopia in the United States between 1971-1972 and 1999-2004. Arch Ophthalmol 2009;127:1632-9.
- Williams KM, Bertelsen G, Cumberland P, et al. Increasing Prevalence of Myopia in Europe and the Impact of Education. Ophthalmology 2015;122:1489-97.
- Dolgin E. The myopia boom. Nature 2015;519:276-8.
- Koh V, Yang A, Saw SM, et al. Differences in prevalence of refractive errors in young Asian males in Singapore between 1996-1997 and 2009-2010. Ophthalmic Epidemiol 2014;21:247-55.
- Holden BA, Fricke TR, Wilson DA, et al. Global Prevalence of Myopia and High Myopia and Temporal Trends from 2000 through 2050. Ophthalmology 2016;123:1036-42.
- Tyler JO, Wagner, H. Myopia Treatments: How to Choose and When to Use? Review of Optometry 2019:46-50.
- Dirani M, Tong L, Gazzard G, et al. Outdoor activity and myopia in Singapore teenage children. Br J Ophthalmol 2009;93:997-1000.
- Guo Y, Liu LJ, Xu L, et al. Outdoor activity and myopia among primary students in rural and urban regions of Beijing. Ophthalmology 2013;120:277-83.
- Jones LA, Sinnott LT, Mutti DO, Mitchell GL, Moeschberger ML, Zadnik K. Parental history of myopia, sports and outdoor activities, and future myopia. Invest Ophthalmol Vis Sci 2007;48:3524-32.
- Lin Z, Vasudevan B, Jhanji V, et al. Near work, outdoor activity, and their association with refractive error. Optom Vis Sci 2014;91:376-82.
- Rose KA, Morgan IG, Ip J, et al. Outdoor activity reduces the prevalence of myopia in children. Ophthalmology 2008;115:1279-85.
- Walline JJ. Myopia Control: A Review. Eye Contact Lens 2016;42:3-8.
- Yeo AC, Atchison DA, Schmid KL. Children’s accommodation during reading of Chinese and English texts. Optom Vis Sci 2013;90:156-63.
- Casson RJ, Gupta A, Newland HS, et al. Risk factors for primary open-angle glaucoma in a Burmese population: the Meiktila Eye Study. Clin Exp Ophthalmol 2007;35:739-44.
- Saw SM, Gazzard G, Shih-Yen EC, Chua WH. Myopia and associated pathological complications. Ophthalmic Physiol Opt 2005;25:381-91.
- Pan CW, Cheng CY, Saw SM, Wang JJ, Wong TY. Myopia and age-related cataract: a systematic review and meta-analysis. Am J Ophthalmol 2013;156:1021-33 e1.
- Chung K, Mohidin N, O’Leary DJ. Undercorrection of myopia enhances rather than inhibits myopia progression. Vision Res 2002;42:2555-9.
- Walline JJ, Jones LA, Mutti DO, Zadnik K. A randomized trial of the effects of rigid contact lenses on myopia progression. Arch Ophthalmol 2004;122:1760-6.
- Cheng D, Woo GC, Drobe B, Schmid KL. Effect of bifocal and prismatic bifocal spectacles on myopia progression in children: three-year results of a randomized clinical trial. JAMA Ophthalmol 2014;132:258-64.
- Guggenheim JA, Northstone K, McMahon G, et al. Time outdoors and physical activity as predictors of incident myopia in childhood: a prospective cohort study. Invest Ophthalmol Vis Sci 2012;53:2856-65.
- Xiong S, Sankaridurg P, Naduvilath T, et al. Time spent in outdoor activities in relation to myopia prevention and control: a meta-analysis and systematic review. Acta Ophthalmol 2017;95:551-66.
- Walline JJ, Greiner KL, McVey ME, Jones-Jordan LA. Multifocal contact lens myopia control. Optom Vis Sci 2013;90:1207-14.
- Ticak A, Walline JJ. Peripheral optics with bifocal soft and corneal reshaping contact lenses. Optom Vis Sci 2013;90:3-8.
- Lam CS, Tang WC, Tse DY, Tang YY, To CH. Defocus Incorporated Soft Contact (DISC) lens slows myopia progression in Hong Kong Chinese schoolchildren: a 2-year randomised clinical trial. Br J Ophthalmol 2014;98:40-5.
- Chia A, Chua WH, Cheung YB, et al. Atropine for the treatment of childhood myopia: safety and efficacy of 0.5%, 0.1%, and 0.01% doses (Atropine for the Treatment of Myopia 2). Ophthalmology 2012;119:347-54.
- Kang P, Swarbrick H. New Perspective on Myopia Control with Orthokeratology. Optom Vis Sci 2016;93:497-503.
- Kang P, Swarbrick H. Peripheral refraction in myopic children wearing orthokeratology and gas-permeable lenses. Optom Vis Sci 2011;88:476-82.
- Weiss RS, Park S. Recent updates on myopia control: preventing progression 1 diopter at a time. Curr Opin Ophthalmol 2019.
- Lipson MJ, Brooks MM, Koffler BH. The Role of Orthokeratology in Myopia Control: A Review. Eye Contact Lens 2018;44:224-30.
- Cheung SW, Boost MV, Cho P. Pre-treatment observation of axial elongation for evidence-based selection of children in Hong Kong for myopia control. Cont Lens Anterior Eye 2018.
- Hiraoka T, Kakita T, Okamoto F, Takahashi H, Oshika T. Long-term effect of overnight orthokeratology on axial length elongation in childhood myopia: a 5-year follow-up study. Invest Ophthalmol Vis Sci 2012;53:3913-9.
- Swarbrick HA, Alharbi A, Watt K, Lum E, Kang P. Myopia control during orthokeratology lens wear in children using a novel study design. Ophthalmology 2015;122:620-30.
- Sun Y, Xu F, Zhang T, et al. Orthokeratology to control myopia progression: a meta-analysis. PLoS One 2015;10:e0124535.
- Si JK, Tang K, Bi HS, Guo DD, Guo JG, Wang XR. Orthokeratology for myopia control: a meta-analysis. Optom Vis Sci 2015;92:252-7.
- Cho P, Cheung SW, Edwards M. The longitudinal orthokeratology research in children (LORIC) in Hong Kong: a pilot study on refractive changes and myopic control. Curr Eye Res 2005;30:71-80.
- Na M, Yoo A. The effect of orthokeratology on axial length elongation in children with myopia: Contralateral comparison study. Jpn J Ophthalmol 2018;62:327-34.











