
March 1, 2022
By Dr. Pavan K. Verkicharla and Mr. Swapnil Thakur
It is important to note that there will be non-responders or slow responders to the treatment. This is where the need for combination treatment strategies is being considered to ensure that ocular growth is regulated swiftly and more effectively.
 Myopia progression and the accompanying axial elongation leading to visually debilitating pathologic retinal conditions concern both eye care professionals and worried parents of myopic children. With the emergence of the pandemic in the year 2019 (COVID-19), the home-confinement policy has begun to serve as a catalyst for even higher myopia progression rates than what is noted in the pre-COVID era, possibly due to a combination of a more indoor-centric lifestyle (digital-ecosystem, involvement in intensive near work activities) and limited outdoor time.1 The current rapid rate of myopia progression in children emphasizes the need for a more aggressive approach in controlling axial elongation.
Myopia progression and the accompanying axial elongation leading to visually debilitating pathologic retinal conditions concern both eye care professionals and worried parents of myopic children. With the emergence of the pandemic in the year 2019 (COVID-19), the home-confinement policy has begun to serve as a catalyst for even higher myopia progression rates than what is noted in the pre-COVID era, possibly due to a combination of a more indoor-centric lifestyle (digital-ecosystem, involvement in intensive near work activities) and limited outdoor time.1 The current rapid rate of myopia progression in children emphasizes the need for a more aggressive approach in controlling axial elongation.
The last decade has seen a boom of myopia and novel interventions to counteract the progression, with global reports of rising myopia prevalence. Various concentrations of topical atropine, bifocal spectacles (prismatic and non-prismatic), progressive addition spectacles, corneal reshaping therapy (orthokeratology), peripheral defocus spectacles (defocus-incorporated multiple segments, highly aspheric lenslet technology), soft contact lenses (center-distance multifocal and extended depth of focus) are currently being widely prescribed to slow the progression of myopia and control ocular growth. While each treatment option is beneficial in controlling myopia progression, none of the environmental, optical, and pharmaceutical anti-myopia treatments either completely inhibit myopia progression or demonstrate the intended therapeutic effect in all individuals.2 It is important to note that there will be non-responders or slow responders to the treatment. This is where the need for combination treatment strategies is being considered to ensure that ocular growth is regulated swiftly and more effectively. As the name suggests, the combination treatment for myopia control should be a combination of any of the two treatment modalities for the sole purpose of controlling axial length.
Atropine with Orthokeratology
The outcomes of recent randomized clinical trials published from the year 2020 onwards have been consistent with the prior research, indicating that a combined treatment (OrthoK with atropine) is more effective than monotherapy (either only OrthoK or atropine) in slowing down myopia progression (see Figure 1). Three randomized clinical trials showed a greater efficacy range of about 56% to 100% in controlling axial elongation in the group treated with the combination of OrthoK with 0.01% atropine than the OrthoK alone: 0.05 ± 0.08 mm vs. -0.01 ± 0.12 mm in six months by Vincent et al.3; 0.07±0.16 mm vs. 0.16 ±0.15 mm in 1 year by Tan et al.4; and 0.40±0.23 mm vs. 0.29 ±0.20 mm in two years by Kinoshita et al.5 Likewise, greater efficacy of 22.8% was reported with a combination of OrthoK and 0.01% atropine than only 0.01% atropine over two years (0.88±0.31D vs. 1.14 ±0.63D).6
While even the three recent meta-analyses7,8,9 suggest atropine combined with OrthoK is more effective in slowing axial elongation than OrthoK or atropine alone, it is worth noting that the effectiveness of combination strategies has so far been tested primarily in children with low to moderate myopia, but not in those with high myopia or high astigmatism. As a result, caution should be exercised before extrapolating or generalizing the findings.
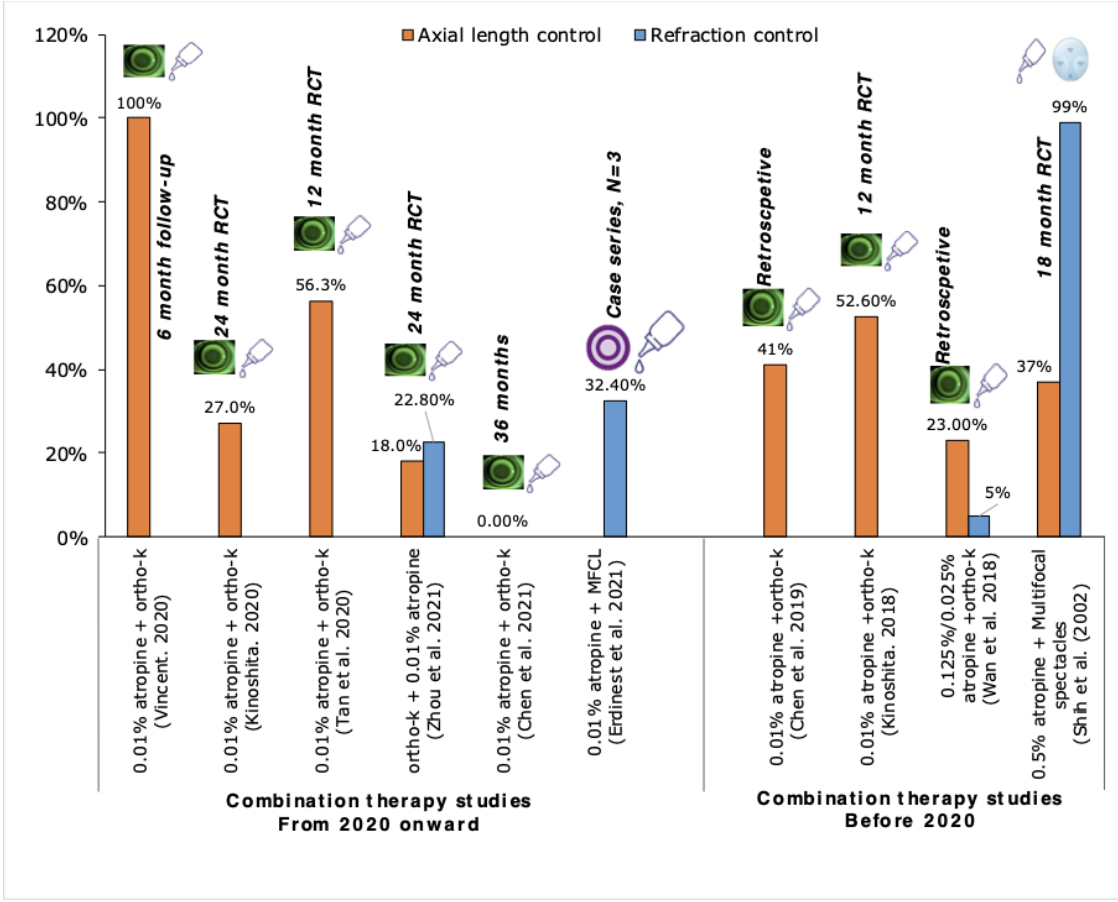
Figure 1: Efficacy of various studies that investigated combination strategies for myopia control. (click to enlarge)
Atropine with Soft Multifocal Contact Lens and “Next-Generation” Spectacle Lenses
Evidence related to combination treatment, including multifocal soft contact lenses or next-generation myopia control spectacle lenses with pharmaceutical treatment, is limited. Preliminary evidence from a recently published case series indicated that one-year treatment with a combination of MiSight 1-day multifocal contact lens and atropine led to slower myopia progression (0.25 ± 0.25D, one-year progression) than the progression rate prior to the treatment (1.12 ± 0.75D, three-year progression).10 With the latest introduction of “next-generation” myopia control lenses, data demonstrates that multisegmented/multifocal defocus lenses such as the MiyoSmart lens with D.I.M.S. technology (HOYA),11 Stellest lens with H.A.L.T. technology (Essilor),12 Myopilux Max lens with +2.00D add and 3D of base-in prism (Essilor),13 are shown to be effective in controlling myopia progression and axial elongation. Although these lenses independently exhibit good efficacy in controlling myopia, it would be interesting to see how these multi-segmented spectacles lenses interact with other anti-myopia strategies during combination treatment. Keep in mind that some non-responders could benefit from the combination strategy.
What to Look for in the Future
Given the multi-factorial nature of myopia etiology, it would be interesting to see how the simple lifestyle modifications (such as spending more hours outdoors and changing the near-work habits) interact with the other optical or pharmacological strategies. Lifestyle modifications such as increasing time outdoors in conjunction with optical or pharmacological intervention are likely recommended by practitioners. Interestingly, data has emerged on the prospective significance of light therapy using specific monochromatic wavelength of light in controlling ocular growth in humans.14-16 Future research should look into how combining light therapy with a specific wavelength would interact with optical or pharmacological strategies. If the light-based strategies work very well, do we still need combination strategies? Maybe — as all humans are not the same, there will still be non-responders. Based on current evidence, it can be expected that the combination of light therapy with any other treatment strategies is likely to increase the overall therapeutic efficacy in controlling the progression (of course, this needs to be tested before application).
Think Before You Act
Certain points need to be considered before starting combination treatment. First, in the case of individuals with a greater risk of myopia progression, the efficacy of monotherapy options for myopia control might drop over time. In such circumstances, the combination treatment (optical plus pharmacological) may be more effective than monotherapy. Second, combination treatment does not mean it would work great for all individuals. Third, any combination treatment is wise to be instituted as a second line of treatment. Keep monotherapy as the first line of treatment even if the myopia progression is rapid. Monitor closely, assess all the possible risk factors, manipulate the strategy and decide on combination when there is an evident progression with monotherapy.
Master — Measure — Monitor — Manage
This is the practical “mantra” that every eye care practitioner needs to follow to treat a juvenile-onset myope successfully.
 |
Dr. Pavan Verkicharla, BS Opt, PhD, is a scientist researching on myopia and heads both the myopia research lab and myopia centre at the L V Prasad Eye Institute, India. Pavan is also a collaborator of BHVI working on myopia-related projects. |
 |
Mr. Swapnil Thakur, BS Opt, PGDOVS, is a research optometrist in the myopia research lab, L V Prasad Eye Institute, India. |
References:
- Wang J, Li Y, Musch DC, Wei N, Qi X, Ding G, et al. Progression of Myopia in School-Aged Children After COVID-19 Home Confinement. JAMA Ophthalmol. 2021;139(3):293-300. Epub 2021/01/15.
- Huang J, Wen D, Wang Q, McAlinden C, Flitcroft I, Chen H, et al. Efficacy Comparison of 16 Interventions for Myopia Control in Children: A Network Meta-analysis. Ophthalmology. 2016;123(4):697-708. Epub 2016/02/02.
- Vincent SJ, Tan Q, Ng ALK, Cheng GPM, Woo VCP, Cho P. Higher order aberrations and axial elongation in combined 0.01% atropine with orthokeratology for myopia control. Ophthalmic Physiol Opt. 2020;40(6):728-37. Epub 2020/09/06.
- Tan Q, Ng AL, Choy BN, Cheng GP, Woo VC, Cho P. One-year results of 0.01% atropine with orthokeratology (AOK) study: a randomised clinical trial. Ophthalmic Physiol Opt. 2020;40(5):557-66. Epub 2020/08/11.
- Kinoshita N, Konno Y, Hamada N, Kanda Y, Shimmura-Tomita M, Kaburaki T, et al. Efficacy of combined orthokeratology and 0.01% atropine solution for slowing axial elongation in children with myopia: a 2-year randomised trial. Sci Rep. 2020;10(1):12750. Epub 2020/07/31.
- Zhou H, Zhao G, Li Y. Adjunctive effects of orthokeratology and atropine 0.01% eye drops on slowing the progression of myopia. Clin Exp Optom. 2021:1-7. Epub 2021/07/07.
- Yang N, Bai J, Liu L. Low concentration atropine combined with orthokeratology in the treatment of axial elongation in children with myopia: A meta-analysis. Eur J Ophthalmol. 2022;32(1):221-8. Epub 2021/03/09.
- Wang S, Wang J, Wang N. Combined Orthokeratology with Atropine for Children with Myopia: A Meta-Analysis. Ophthalmic Res. 2021;64(5):723-31. Epub 2020/08/12.
- Gao C, Wan S, Zhang Y, Han J. The Efficacy of Atropine Combined With Orthokeratology in Slowing Axial Elongation of Myopia Children: A Meta-Analysis. Eye Contact Lens. 2021;47(2):98-103. Epub 2020/10/17.
- Erdinest N, London N, Levinger N, Morad Y. Myopia Control with Combination Low-Dose Atropine and Peripheral Defocus Soft Contact Lenses: A Case Series. Case Rep Ophthalmol. 2021;12(2):548-54. Epub 2021/07/13.
- Lam CSY, Tang WC, Tse DY, Lee RPK, Chun RKM, Hasegawa K, et al. Defocus Incorporated Multiple Segments (DIMS) spectacle lenses slow myopia progression: a 2-year randomised clinical trial. Br J Ophthalmol. 2020;104(3):363-8. Epub 2019/05/31.
- Bao J, Yang A, Huang Y, Li X, Pan Y, Ding C, et al. One-year myopia control efficacy of spectacle lenses with aspherical lenslets. Br J Ophthalmol. 2021. Epub 2021/04/04.
- Cheng D, Woo GC, Drobe B, Schmid KL. Effect of bifocal and prismatic bifocal spectacles on myopia progression in children: three-year results of a randomized clinical trial. JAMA Ophthalmol. 2014;132(3):258-64. Epub 2014/01/18.
- Thakur S, Dhakal R, Verkicharla PK. Short-Term Exposure to Blue Light Shows an Inhibitory Effect on Axial Elongation in Human Eyes Independent of Defocus. Invest Ophthalmol Vis Sci. 2021;62(15):22. Epub 2021/12/23.
- Jiang Y, Zhu Z, Tan X, Kong X, Zhong H, Zhang J, et al. Effect of Repeated Low-Level Red-Light Therapy for Myopia Control in Children: A Multicenter Randomized Controlled Trial. Ophthalmology. 2021. Epub 2021/12/06.
- Torii H, Kurihara T, Seko Y, Negishi K, Ohnuma K, Inaba T, et al. Violet Light Exposure Can Be a Preventive Strategy Against Myopia Progression. EBioMedicine. 2017;15:210-9. Epub 2017/01/09.











