
Jan. 2, 2020
By Krupa Philip, BOptom, PhD
Brien Holden Vision Institute
 Myopia, a growing public health concern, has been rising in prevalence with almost 50% of the world’s population estimated to be myopic by the year 20501. Sight threatening complications such as cataract, glaucoma, vitreous liquefaction, and a range of retinal and macular anomalies known as myopic maculopathy could occur as a result of high myopia (worse than -6.00 D). Younger ages are associated with greater annual progression and thus, early-onset myopia is likely to result in higher levels of final net myopia2. It is, therefore critical to curb the burden of myopia through strategies aimed to control and slow the progression of myopia. There now exist several optical and pharmacological interventions to slow myopia. Presently, optical interventions for myopia control include peripheral defocus correcting spectacle lenses, bifocal spectacles, progressive addition spectacles, multifocal soft contact lenses and orthokeratology3. Of these, single vision spectacles designed to alter peripheral defocus demonstrated only a small treatment effect, less than 14% reduction in myopia progression4. Bifocal and progressive addition spectacles demonstrated variable treatment effect (6% to 51%) in reducing the progression of myopia. Among the optical interventions, orthokeratology (30% to 50%) and multifocal soft contact lenses (centre-distance multifocal contact lenses – 38%) showed promising results in slowing myopia progression.
Myopia, a growing public health concern, has been rising in prevalence with almost 50% of the world’s population estimated to be myopic by the year 20501. Sight threatening complications such as cataract, glaucoma, vitreous liquefaction, and a range of retinal and macular anomalies known as myopic maculopathy could occur as a result of high myopia (worse than -6.00 D). Younger ages are associated with greater annual progression and thus, early-onset myopia is likely to result in higher levels of final net myopia2. It is, therefore critical to curb the burden of myopia through strategies aimed to control and slow the progression of myopia. There now exist several optical and pharmacological interventions to slow myopia. Presently, optical interventions for myopia control include peripheral defocus correcting spectacle lenses, bifocal spectacles, progressive addition spectacles, multifocal soft contact lenses and orthokeratology3. Of these, single vision spectacles designed to alter peripheral defocus demonstrated only a small treatment effect, less than 14% reduction in myopia progression4. Bifocal and progressive addition spectacles demonstrated variable treatment effect (6% to 51%) in reducing the progression of myopia. Among the optical interventions, orthokeratology (30% to 50%) and multifocal soft contact lenses (centre-distance multifocal contact lenses – 38%) showed promising results in slowing myopia progression.
Pharmacological interventions for myopia control include Atropine, Pirenzepine, 7-Methylxanthine and Timolol3. Of these, Atropine is the most widely used, with higher concentrations more effective (dose-dependent). Atropine 1% concentration demonstrated 60% to 80% reduction in progression of myopia. However, the side effects associated with higher concentrations, such as loss of accommodation, photophobia, etc. make it a less appealing myopia treatment option.
Behavioral interventions such as increased time outdoors, less near work activities, and improved lighting indoors are considered protective against myopia incidence and somewhat effective against progression3.
In spite of the multiple options available, in certain circumstances, individual interventions may not result in the expected efficacy. In such situations, may need to resort to switching treatments, considering higher doses of the intervention, or consider a combination strategy.
With respect to combination strategies, available data is limited, but presently there are a number of randomized clinical trials in progress to assess the efficacy of combination treatment for myopia control. Importantly, the few studies that assessed the effects of combination strategies show promising results. A randomized controlled trial conducted in the early 2000s found a significant reduction of myopia progression with the combination of 0.5% atropine and progressive addition lenses (PALS) in children aged 6 to 13 years5. The mean progression of myopia was significantly less in the combination group of atropine and PALS (0.41D) compared to 1.19D with PALS and 1.40D with single vision spectacles5.
More recently, the effects of combination therapy of low dose atropine (0.125% and 0.025%) and orthokeratology were evaluated and compared to orthokeratology treatment alone6. Lesser axial length elongation and myopic shift in refractive error were observed with the combination therapy compared to the orthokeratology group6. However, the information from this study was limited due to the retrospective design and non-randomization of study participants. However, a further 2-year clinical trial investigated the efficacy of atropine 0.01% combined with orthokeratology and reported an improved treatment outcome of more than 50%7. The combination treatment reduced axial elongation by 50% compared to the control group7. Table 1 details the studies investigating combination therapies on myopia progression.
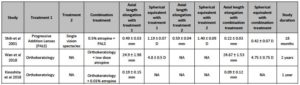
Table 1. Details of studies investigating combination therapies on myopia progression. NA – information not available.
Additionally, efforts are underway to improve the efficacy of low dose atropine without associated side effects such as with the use of extended drug release systems. In this respect, contact lenses offer the advantage of serving as a drug release platform and also may contribute to efficacy via optical mechanisms. A study by Hui et al. reported both multifocal and non-multifocal contact lenses of the same materials released the same amount of atropine and pirenzepine over the course of 24 hours8.
Encouragingly, other clinical trials investigating the effect of combination treatment on myopia control are underway. One example is the BAM study investigating the effect of 0.01% atropine and +2.50D add center distance bifocal soft contact lenses9. Furthermore, behavioral modifications such as increased outdoor time could be implemented along with other optical strategies to improve the myopia control treatment efficacy.
In summary, the knowledge base is encouraging for combination strategies involving optical, pharmaceutical and behavioral modifications to prevent or slow myopia progression.
Krupa Philip, BOptom, PhD, is a research scientist with the Brien Holden Vision Institute.
REFERENCES
- Holden, B.A., et al., Myopia: a growing global problem with sight-threatening complications. Community Eye Health, 2015. 28(90): p. 35.
- Sankaridurg, P., A less myopic future: what are the prospects? Clin Exp Optom, 2015. 98(6): p. 494-6.
- Wildsoet, C.F., et al., IMI – Interventions Myopia Institute: Interventions for Controlling Myopia Onset and Progression Report. Invest Ophthalmol Vis Sci, 2019. 60(3): p. M106-M131.
- Wolffsohn, J.S., et al., IMI – Myopia Control Reports Overview and Introduction. Invest Ophthalmol Vis Sci, 2019. 60(3): p. M1-M19.
- Shih, Y.F., et al., An intervention trial on efficacy of atropine and multi-focal glasses in controlling myopic progression. Acta Ophthalmol Scand, 2001. 79(3): p. 233-6.
- Wan, L., et al., The Synergistic Effects of Orthokeratology and Atropine in Slowing the Progression of Myopia. J Clin Med, 2018. 7(9).
- Kinoshita, N., et al., Additive effects of orthokeratology and atropine 0.01% ophthalmic solution in slowing axial elongation in children with myopia: first year results. Jpn J Ophthalmol, 2018. 62(5): p. 544-553.
- Hui, A., et al., In vitro release of two anti-muscarinic drugs from soft contact lenses. Clin Ophthalmol, 2017. 11: p. 1657-1665.
- Huang, J., et al., Bifocal & Atropine in Myopia Study: Baseline Data and Methods. Optom Vis Sci, 2019. 96(5): p. 335-344.











