
October 16, 2023
By Alex Ong, OD, FAAO

goc, Getty Images
Subjective
SO, a 9-year-old Chinese female, came for an eye examination at our practice in August 2022 due to failing the school’s health vision screening. Prior to this visit, SO had not undergone any eye examinations as she had not reported any vision-related concerns. Upon conducting a visual acuity check, it was observed that SO had an unaided visual acuity (VA) of 6/12-2 monocularly.
Objective
Retinoscopy:
RE: -1.00/-1.50 x 180 VA: 6/7.5
LE: -1.00/-1.25 x 180 VA: 6/7.5
Non-Cycloplegic Subjective Refraction:
RE: -1.50/-1.50 x 180 VA: 6/6
LE: -1.50/-1.25 x 180 VA: 6/6
Axial Length using IOL Master 500
RE: 25.92 mm
LE: 25.63 mm
Diagnosis
Although the spherical equivalent refraction is minimal, it does not align with her axial length. Judging by her axial length measurement, she is approaching a state of high myopia.1 Despite the modest refractive myopia, her axial length is significantly longer than the average, warranting a more proactive approach to myopia management. Even a minor 0.25D increase in myopia can have a notable impact on her condition. Effective myopia management should encompass the following considerations:
- Providing education regarding potential ocular complications associated with an elongated axial length.
- Highlighting the urgent need for myopia management in the case of SO to mitigate the risk of further progression.
- Presenting available options for myopia management and summarizing research findings regarding their success rates.
- Emphasizing the importance of regular follow-ups every three months during the initial year of treatment to monitor the progression rate.
In Singapore, optometrists are able to offer various myopia management options, including:
1.Ophthalmic Lenses:
- MiYOSMART (HOYA Vision Care)
- Stellest (EssilorLuxottica)
2. Soft Contact Lenses:
- MiSight (CooperVision)
- Bloom Day (Menicon)
- ACUVUE Abiliti 1 day (Johnson & Johnson Vision)
3. Cornea Reshaping
- Orthokeratology
These options are available for the management and control of myopia, and optometrists can recommend and fit patients with the most suitable option based on their specific needs and conditions.
The treatment involving atropine, in Singapore, is exclusively administered by ophthalmologists, and it was indeed discussed as an option. However, parents tend to lean towards the use of spectacles as they perceive contact lenses, in any form, to be associated with a risk of blinding complications.
Plan
Consequently, peripheral defocus lenses (Stellest) were recommended and prescribed for SO.
Follow-up Review
SO only came in for a follow-up appointment 11 months after receiving her spectacles. The parents noted that SO had not reported any complaints of blurred vision when asked, leading them to delay seeking a review. However, more recently, SO failed the school vision screening test, revealing a VA of 6/9 for each eye.
Retinoscopy:
RE: -2.25/-1.75 x 180 VA: 6/7.5
LE: -2.25/-1.75 x 180 VA: 6/7.5
Non-Cycloplegic Subjective Refraction:
RE: -2.75/-1.75 x 180 VA: 6/6
LE: -2.75/-1.75 x 180 VA: 6/6
Axial Length (MOPTIM Colombo Biometer)
RE: 26.34 mm
LE: 26.07 mm
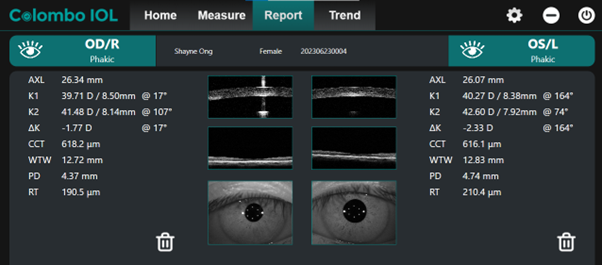
Figure 1: Ocular Biometry of SO before starting OrthoK lenses
Given the significant axial elongation of both eyes to 26 mm, it was strongly advised to the parent that managing SO’s myopia with spectacles might not be the most effective solution. It was observed that SO’s spectacles were drooping down, causing her to primarily use the superior part of the ophthalmic lenses, likely contributing to the observed poor efficacy. Due to this issue in wearing the spectacles properly within the treatment zone, OrthoK was strongly recommended, as it has shown high efficacy in controlling myopia.2 Additionally, OrthoK would ensure that SO’s treatment area is correctly placed.
SO’s astigmatism was notably high, making it impractical to correct it effectively using myopia management soft contact lenses. Alternatively, to enhance the effectiveness of myopia management, a combined approach involving atropine and OrthoK was suggested, as research indicates its potential for improved myopia management.3
SO was enrolled in the OrthoK treatment plan without the addition of atropine. Specifically, she was fitted with Bloom Night OrthoK lenses, which have received CE approval for safe wear and are designed for myopia management in children with prescriptions up to -4.00D.4 The Bloom Night treatment regimen promotes the replacement of lenses every six months, enhancing safety and cleanliness in OrthoK lens wear for SO. Moreover, this schedule helps to reassure the parent regarding the safety of the treatment and encourages them to bring SO for regular three-month follow-up reviews, which entitle SO to lens replacements as part of the treatment program.
SO demonstrated good tolerance and adaptation to the OrthoK lenses, experiencing no major issues with lens centration. Remarkably, within just one week of wearing the OrthoK lenses, her refractive error was completely corrected, yielding the following prescription:
Non-Cycloplegic Subjective Refraction:
RE: Plano VA: 6/6
LE: Plano VA: 6/6
Retinoscopy:
RE: +0.75D VA: 6/7.5
LE: +0.50D VA: 6/7.5
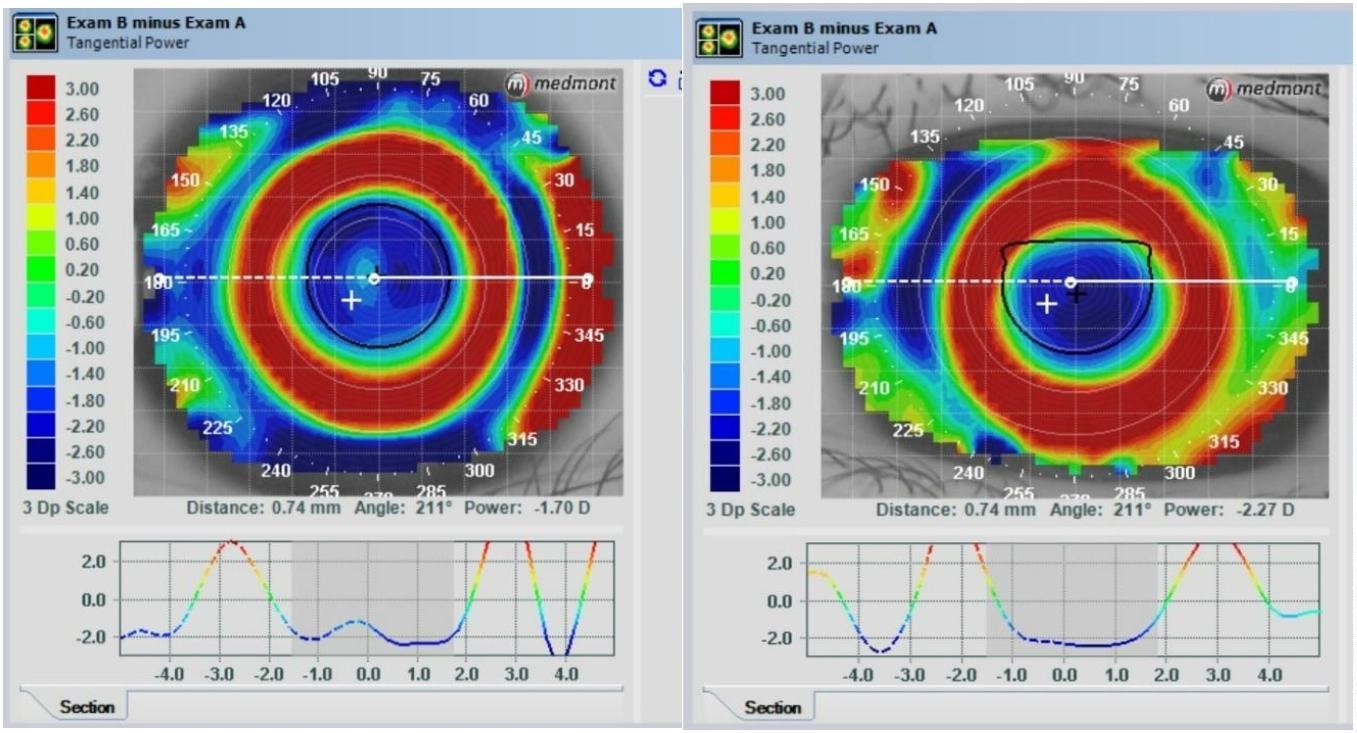
Figure 2: One week after wearing Bloom Night OrthoK lenses. (Click to enlarge.)
Three and six-month review of SO shows that refraction did not increase, and axial length remained very stable.
Discussion
Singapore holds one of the highest rates of myopia globally, with a staggering 65% of students being affected by myopia by the age of 12. Additionally, the prevalence of severe defective vision due to myopia stands at 13%.5 Given these concerning statistics, myopia management has garnered significant attention and interest among eye care practitioners in Singapore. Efforts to address and mitigate myopia are of paramount importance to the eye health and well-being of the population, especially among the younger demographic.
The decision regarding the appropriate mode of myopia management can vary significantly, primarily based on the individual’s ocular condition. In the case of SO, despite her considerably low refractive error, her axial length indicated a highly myopic condition. This highlights the critical role of ocular biometry in accurately assessing the severity of myopia and determining the appropriate course of treatment. Relying solely on refractive error and age to guide treatment decisions can lead to a higher risk of mismanagement, potentially delaying necessary interventions.6 Parents might perceive a low refractive prescription as less urgent, inadvertently delaying crucial steps to slow myopia progression. This underscores the importance of not relying on refraction alone and emphasizes the need for a comprehensive assessment, including ocular biometry, to inform effective myopia management strategies.
Hence, its’ evident that the correlation between refraction and axial length may not be strong. I recommend that when the axial length significantly exceeds the usual range for a particular age group (≥75th percentile), or when the axial length approaches approximately 26mm, even with a low refractive error, an assertive approach involving interventions such as OrthoK and/or atropine treatment should be strongly advocated. This proactive stance is crucial for timely interventions and effective management of ocular changes associated with myopia.
Certainly, the restrictions on using pharmacological drugs for diagnosis and treatment in Singapore pose a challenge for monitoring myopia progression. Consequently, relying on ocular biometry has become fundamental in myopia management within the optometric scope. However, achieving precise and repeatable measurements is crucial, given the limited attention span and potential fixation issues, particularly in pediatric patients.7 Off-axis measurements of axial length can introduce inaccuracies and misinterpretations of ocular growth, underscoring the need for meticulous technique and patient cooperation during biometry assessments. The accuracy and reliability of these measurements are paramount in guiding appropriate myopia management strategies.
Absolutely, advancements in ocular biometry have significantly enhanced the precision and reliability of axial length measurements. The ability to visualize a specific 3mm section of OCT imaging of the retina, precisely aligned with the macular region, ensures that axial length measurements are highly accurate and consistent. This technology greatly aids in educating parents about myopia management by providing tangible, data-driven results before and after treatment. It also instills confidence in optometrists, assuring them of the reliability of these measurements, especially in the absence of wet refraction. These technological capabilities play a crucial role in optimizing myopia management strategies and fostering better communication with both parents and practitioners.
In conclusion, relying solely on refractive error to determine the mode of myopia treatment is inadequate. Ocular biometry with precise measurements plays a pivotal role in accurately diagnosing and monitoring myopia management, particularly in cases involving a flat cornea with an elongated ocular axial length. The integration of advanced biometric technologies ensures a comprehensive understanding of ocular conditions, allowing for tailored and effective interventions to mitigate myopia progression and promote better eye health.
 |
Dr. Alex Ong is a clinical optometrist with a passion for myopia management, contact lenses, and binocular vision. He is the second generation owner of Ong’s Optics & Contact Lens Center and Founder of Ong’s Optics Myopia Management Center. Dr Ong graduated with a Diploma in Optometry (Merit) from Singapore Polytechnic. He also got his BSc in Optometry and MSc in Clinical Optometry from Salus University. Dr. Ong further completed his Optometry Doctorate at Aston University in 2018 and published his research thesis on multifocal contact lenses and ocular fatigue among esophoric and orthophoric myopes. He is also a Fellow with the American Academy of Optometry. Dr. Ong formerly lectured at Singapore Polytechnic and Ngee Ann Polytechnic. He was also a Key Opinion Leader for Alcon Singapore. His vast experience in myopia management with ophthalmic lenses and orthokeratology allows him to lecture in Singapore, Malaysia, and Indonesia. |
References
1 Kim H.Y., Kim S.S., Factors associated with axial length elongation in high myopia in adults, Int J Ophthal, 2021; 14(8): 1231-1236.
2 Hiraoka T., Myopia Control with orthokeratology: A review, Eye Con Lens, 2022, 48(3): 100-104
3 Tsai H.R., Wang J. H, Huang H.K, Chen T. L., Chen P. W., Chiu C. J., Efficacy of atropine, orthokeratology and combined atropine with orthokeratology for childhood myopia: A systematic review and network meta-analysis, J. Formos Med Assoc, 121(12):2490-2500.
4 WHITE PAPER ON Menicon Bloom Myopia Control Management System, 2022, https://www.menicon.com/menicon-bloom/downloads/white-paper.pdf
5 Karuppiah V., Wong L., Tay V., Ge X., Kang L.L., School-based programme to address childhood myopia in Singapore, 2021, Singapore Med J., 62(2): 63-68.
6 Vera-Diaz F.A, The importance of measuring axial length, https://reviewofmm.com/the-importance-of-measuring-axial-length-when-managing-childhood-myopia/
7 Sahin A., Hamrah P., Clinically relevant Biometry, CurrO pin Ophthalmol, 2012, 23(1): 47-53.











