
July 1, 2021
By Thomas Aller, OD, FBCLA, Collaborating Scientist, Brien Holden Vision Institute
The value of monitoring axial length change with optical biometers in myopia management is that the measurements are highly accurate so that clinicians can make rational decisions to improve treatment efficacy.

It is widely acknowledged that myopia has significantly increased in its prevalence worldwide1 and that uncontrolled progression leads to increased risks of ocular pathology linked to axial elongation.2 After a mere 30 years of accumulating evidence of effective means for myopia control, several authoritative bodies such as the American Optometric Association, American Academy of Ophthalmology, and the World Council of Optometry have recently declared that the new standard of care for myopia must include early detection of children at risk, a complete discussion with parents and patients of appropriate age, and managing myopia progression with evidence-based treatments either directly or via referral or co-management.3
That is not to say that there are no arguments left in the field, but there is a broad consensus developing that myopia progression should be managed rather than just observed. A remaining area of contention has to do with how myopia management should be diagnosed and monitored. Figure 1 illustrates the advantages and disadvantages of managing myopia with refractive monitoring versus biometric monitoring. Indeed, the best way to diagnose myopia is with refractive error, and the best way to monitor progression is to measure axial length with an optical biometer.
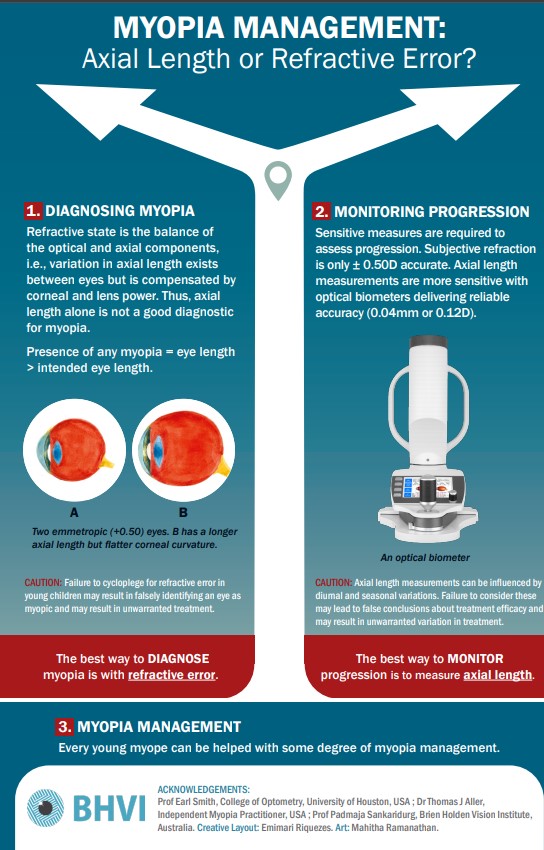
Figure 1
The pathology related to myopia progression must undoubtedly be caused by excess axial elongation rather than corneal curvature changes or lenticular changes, so the fundamental goal of myopia management must be to lessen axial elongation. While it is certainly true that in most cases of childhood myopia progression, refractive change is highly correlated with axial elongation4, there are many potential advantages to routinely measuring axial length.
This paper will explore the predictive value of axial length measurement, how one should interpret changes in axial length, and how that interpretation might change based on several factors. These include age, level of myopia, the season, and how monitoring axial elongation might allow for more precise tailoring of the treatment approach to maximize outcomes.5
The Benefits of Centile Curves for Myopia Management
While growth curves have been common for assessing height and weight in pediatric populations6, axial length and refractive curves have only recently become available.7-9 Such centile curves help evaluate the risk of developing myopia or high myopia based on axial length measurements at a particular age. Several optical biometers have been recently introduced that incorporate software for monitoring, tracking, and projecting axial changes over time from Haag-Streit, Oculus, and Topcon. The more confident a practitioner can be that an individual child is likely to develop myopia in the future (a state now defined as pre-myopia10), the more confidence there can be in instituting various preventive strategies, including atropine, novel spectacle-based approaches, and lifestyle recommendations related to near work and outdoor time.
It has been argued that, in the absence of studies demonstrating changes in myopia control efficacy when switching a patient from one treatment to another, there is no reason ever to change a treatment decision. While that may be a valid academic argument, it is unnecessarily restrictive in clinical practice. Most practitioners would expect that most treatments are likely to follow a dose-response relationship, and they would reasonably assume it to be the same for myopia. In a case series in the author’s practice, 157 cases were identified in which there were changes in treatment method or presumed effectiveness. Myopia control efficacy was found to increase significantly with increased treatment strength and was relatively neutral with a neutral change, and efficacy was minimally worse with decreased treatment effect.11 While not more than suggestive of the dose-response effect, this case series offers some confidence to the practitioner that there may be value in precisely measuring myopia/axial length progression and adjusting the treatment strength as necessary depending on whether the outcomes match the outcome goals.
The value of monitoring axial length change with optical biometers in myopia management is that the measurements are highly accurate so that clinicians can make rational decisions to help to improve treatment efficacy. Since myopia progression tends to follow seasonal patterns12, caution must be exercised to avoid either making an unwarranted treatment change based on a seasonal increase in axial length or to avoid ascribing to the new treatment the improvement in efficacy better accounted for by a seasonal dip in axial elongation.
Emmetropic children also experience axial elongation13, and this presumed normal physiologic growth has to be taken into account when assessing the meaning of observed axial growth during myopia management. Expected emmetropic axial length can be estimated by using the formula provided in this referenced paper13, converted here to work in a spreadsheet: =IF(AGECELL#<10.5,20.189+(1.258*LN(AGECELL#)),IF(AGECELL#>10.49,21.353+(0.759*LN(AGECELL#)))), in which AGECELL# is the cell containing the age of the patient, and LN is the natural logarithm. This can calculate the expected annual growth or rate by adding measurement data and duration between treatments.
Interpreting Axial Length Measurements
In summary, axial length growth curves can help identify patients at risk for future myopia and allow early interventions for better final outcomes. Routinely monitoring axial length changes during treatment can allow for more timely modifications of treatment strategies and better long-term results. How to properly analyze the meaning of axial length changes is where it gets a bit tricky. The most straightforward result to explain is when axial length growth slows to zero or reduces slightly after treatment. That is an obvious sign of treatment success, particularly in younger patients. At some point during the aging process, natural growth slows, and zero growth under treatment may simply be the equivalent of stepping on the brakes when the car is standing still. Another easily interpreted result is when axial length either does not slow or accelerates after treatment, as that is likely evidence that the treatment is not working.
On the other hand, mildly effective treatments imposed at the beginning of fall or winter may still be associated with increased axial length compared to the prior summer period since myopia accelerates in the winter. More difficult to explain to parents is when the eyes continue to grow after telling them that myopia management aims to slow the excess growth. When this growth matches or is less than the predicted emmetropic axial growth for the same age child, this is likely excellent clinical success.14

Thomas Aller, OD, FBCLA, collaborates with the Brien Holden Vision Institute and is a Visiting Scholar at the University of California, Berkeley School of Optometry. He practices in San Bruno, Calif.
References
- Holden BA, Fricke TR, Wilson DA, et al. Global Prevalence of Myopia and High Myopia and Temporal Trends from 2000 through 2050. Ophthalmology. May 2016;123(5):1036-42. doi:10.1016/j.ophtha.2016.01.006
- Flitcroft DI. The complex interactions of retinal, optical and environmental factors in myopia aetiology. Prog Retin Eye Res. Nov 2012;31(6):622-60. doi:10.1016/j.preteyeres.2012.06.004
- Modjtahedi BS, Abbott RL, Fong DS, Lum F, Tan D, Myopia TFo. Reducing the Global Burden of Myopia by Delaying the Onset of Myopia and Reducing Myopic Progression in Children: The Academy’s Task Force on Myopia. Ophthalmology. Dec 2020;doi:10.1016/j.ophtha.2020.10.040
- Gwiazda J, Marsh-Tootle WL, Hyman L, Hussein M, Norton TT, Group CS. Baseline refractive and ocular component measures of children enrolled in the correction of myopia evaluation trial (COMET). Invest Ophthalmol Vis Sci. Feb 2002;43(2):314-21.
- Cruickshank FE, Logan NS. Optical ‘dampening’ of the refractive error to axial length ratio: implications for outcome measures in myopia control studies. Ophthalmic Physiol Opt. 05 2018;38(3):290-297. doi:10.1111/opo.12457
- Niklasson A, Ericson A, Fryer JG, Karlberg J, Lawrence C, Karlberg P. An update of the Swedish reference standards for weight, length and head circumference at birth for given gestational age (1977-1981). Acta Paediatr Scand. 1991 Aug-Sep 1991;80(8-9):756-62. doi:10.1111/j.1651-2227.1991.tb11945.x
- Tideman JWL, Polling JR, Vingerling JR, et al. Axial length growth and the risk of developing myopia in European children. Acta Ophthalmol. May 2018;96(3):301-309. doi:10.1111/aos.13603
- Sanz Diez P, Yang LH, Lu MX, Wahl S, Ohlendorf A. Growth curves of myopia-related parameters to clinically monitor the refractive development in Chinese schoolchildren. Graefes Arch Clin Exp Ophthalmol. May 2019;257(5):1045-1053. doi:10.1007/s00417-019-04290-6
- McCullough S, Adamson G, Breslin KMM, McClelland JF, Doyle L, Saunders KJ. Axial growth and refractive change in white European children and young adults: predictive factors for myopia. Sci Rep. 09 2020;10(1):15189. doi:10.1038/s41598-020-72240-y
- Flitcroft DI, He M, Jonas JB, et al. IMI – Defining and Classifying Myopia: A Proposed Set of Standards for Clinical and Epidemiologic Studies. Invest Ophthalmol Vis Sci. 02 2019;60(3): M20-M30. doi:10.1167/iovs.18-25957
- Aller T. Real World Myopia Management: When and How to Change Treatments. Review of Myopia Management. June 1, 2020.
- Donovan L, Sankaridurg P, Ho A, et al. Myopia progression in Chinese children is slower in summer than in winter. Optom Vis Sci. Aug 2012;89(8):1196-202. doi:10.1097/OPX.0b013e3182640996
- Zadnik K, Mutti DO, Mitchell GL, Jones LA, Burr D, Moeschberger ML. Normal eye growth in emmetropic schoolchildren. Optom Vis Sci. Nov 2004;81(11):819-28. doi:10.1097/01.opx.0000145028.53923.67
- Chamberlain P, Lazon de la Jara P, Arumugam B, Bullimore MA. Axial length targets for myopia control. Ophthalmic Physiol Opt. 05 2021;41(3):523-531. doi:10.1111/opo.12812











