
June 1, 2021
By Rebecca Weng, BOptom (Hons), Grad Dip(I&T), MBA; Programs and Partnership Liaison Director, Myopia Program Facilitator, and Project Manager Brien Holden Vision Institute
The decision to discontinue myopia treatment requires as much consideration as treatment initiation. However, close monitoring is mandatory in managing these patients.

While there are many studies reporting on the efficacy of various myopia control options, the “when” and “how” to discontinue an individual from myopia management options are not well understood. Many factors may drive discontinuation of myopia management treatment; for example, non-adherence to treatment strategy, an individual’s circumstances (for example, relocating to a place where a specific myopia treatment may not be available), a change in myopia profile, or more commonly by stable myopia. Understanding when, how, and any related risks (for example, rebound effects) may aid the practitioner in managing the situation appropriately.
When to Stop Myopia Management Treatment
Different considerations may apply when considering an optical strategy as opposed to a pharmaceutical approach. All else being similar, the time at which myopia treatment can be discontinued applies similarly for both strategies and is based both on the patient’s age and the rate of change of refractive error. Myopia progression generally slows during late adolescence/early adulthood. However, for a given eye, the age at which progression slows to a minimum or stops is uncertain. In some eyes, myopia stabilization may not occur until the 20s.1 Therefore, the practitioner may have to rely on both factors, i.e., age and stability, to decide on discontinuation. Although there are no clear guidelines, no or minimal change in refractive error over 1.5 to 2 years may indicate that the progression is minimal to stable. However, it may be important to consider the patient’s age when deciding — for example, even if a 12-year-old has not changed in refractive error, would they be deemed stable?2 While such a determination may be made with more confidence in an older individual, there may need to be a subsequent period of observation in a younger eye to evaluate any risk of future progression.
How to Stop Myopia Management Treatment
With an optical approach, switching to a suitable corrective modality, i.e., either contact lens or spectacles based on the motivation, cost, etc., may be indicated.
With topical atropine, there has been a move to tapering in recent years rather than simply discontinuing due to a “rebound phenomenon.” With atropine, the treatment effect is dose dependent, and there is also an inverse dose-related increase in myopia progression upon cessation of treatment.3-5 Chia et al. proposed an initial two-year treatment period using 0.01% atropine. If there is no progression of <0.25D in the second year, then atropine could be stopped and children monitored.5 If an increase in progression occurs, restart treatment for a further period until the progression slows to <0.25D /year.5
Wu et al. advise a more conservative approach by decreasing dose and monitoring progression (Figure 1).6 Close monitoring after treatment cessation is required so that any noticeable acceleration in progression can be quickly addressed by the reintroduction of 0.01% atropine and behavior modification.6 Tapering by decreasing frequency was also suggested as an alternative.7
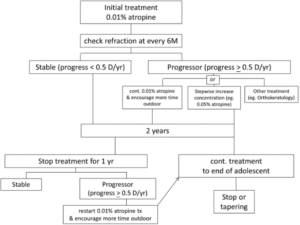
Figure 1. Clinical implementation of atropine treatment model proposed by Wu et al.6
Considerations Post Discontinuation
Closer monitoring may be needed in the months following discontinuation to determine any reversal of stability and/or increasing progression more than normal (rebound). Although rebound needs to be considered for both optical and pharmaceutical strategies, it appears to be a stronger factor for pharmaceutical approaches.
Cho et al. noticed an accelerated axial elongation rate during the discontinuation phase of orthokeratology lens wear; however, this effect was reversed upon lens wear resumption.8 This led them to conclude that early termination of OrthoK lens wear is not recommended. If lens wear is discontinued, monitor axial length change every three months, with lens wear resumed as soon as accelerated axial elongation is detected. In contrast, Berntsen et al. found that the treatment effect was not lost upon PAL discontinuation. However, it is unclear whether this treatment effect will remain indefinitely.9 Cheung et al. reported no rebound effect following the discontinuation of novel soft contact lenses.10 And recently, the results of a study on dual-focus soft contact lenses showed a continued treatment effect over a 6-year period.11
In summary, the decision to discontinue myopia treatment requires as much consideration as treatment initiation. Treatment cessation may be best carried out when the myopia progression rate slows, which is usually when the child reaches late adolescence.1,12,13 However, close monitoring is mandatory in managing these patients. If acceleration in myopia progression is detected, immediate recommencement of treatment is required.

Rebecca Yan Shun Weng BOptom (Hons), GradCert OcTher, GradDip I&T, NAATI (Translator) is a project manager with BHVI. Her areas of interest are myopia, contact lenses, clinical trials, and partnership engagement.
Reference
- Myopia stabilization and associated factors among participants in the Correction of Myopia Evaluation Trial (COMET). Invest Ophthalmol Vis Sci 2013;54(13):7871-84. doi: 10.1167/iovs.13-12403 [published Online First: 2013/10/26]
- Gifford KL, Richdale K, Kang P, et al. IMI – Clinical Management Guidelines Report. Invest Ophthalmol Vis Sci 2019;60(3): M184-m203. doi: 10.1167/iovs.18-25977 [published Online First: 2019/03/01]
- Tong L, Huang XL, Koh AL, et al. Atropine for the treatment of childhood myopia: effect on myopia progression after cessation of atropine. Ophthalmology 2009;116(3):572-9. doi: 10.1016/j.ophtha.2008.10.020 [published Online First: 2009/01/27]
- Chia A, Chua WH, Wen L, et al. Atropine for the treatment of childhood myopia: changes after stopping atropine 0.01%, 0.1% and 0.5%. Am J Ophthalmol 2014;157(2):451-57.e1. doi: 10.1016/j.ajo.2013.09.020 [published Online First: 2013/12/10]
- Chia A, Lu QS, Tan D. Five-Year Clinical Trial on Atropine for the Treatment of Myopia 2: Myopia Control with Atropine 0.01% Eyedrops. Ophthalmology 2016;123(2):391-99. doi: 10.1016/j.ophtha.2015.07.004 [published Online First: 2015/08/15]
- Wu PC, Chuang MN, Choi J, et al. Update in myopia and treatment strategy of atropine use in myopia control. Eye (Lond) 2019;33(1):3-13. doi: 10.1038/s41433-018-0139-7 [published Online First: 2018/06/13]
- Brenner RL. Further observations on use of atropine in the treatment of myopia. Ann Ophthalmol 1985;17(2):137-40. [published Online First: 1985/02/01]
- Cho P, Cheung SW. Discontinuation of orthokeratology on eyeball elongation (DOEE). Cont Lens Anterior Eye 2017;40(2):82-87. doi: 10.1016/j.clae.2016.12.002 [published Online First: 2017/01/01]
- Berntsen DA, Sinnott LT, Mutti DO, et al. A randomized trial using progressive addition lenses to evaluate theories of myopia progression in children with a high lag of accommodation. Invest Ophthalmol Vis Sci 2012;53(2):640-9. doi: 10.1167/iovs.11-7769 [published Online First: 2011/12/30]
- Cheng X, Xu J, Chehab K, et al. Soft Contact Lenses with Positive Spherical Aberration for Myopia Control. Optom Vis Sci 2016;93(4):353-66. doi: 10.1097/opx.0000000000000773 [published Online First: 2015/12/26]
- Chamberlain P LN, Jones D, Gonzalez-Meijome J, Saw S-M, Young G. Clinical evaluation of a dual-focus myopia control 1 day soft contact lens: 6-year results. 2020 American Academy of Optometry Annual Meeting 2020
- Thorn F, Gwiazda J, Held R. Myopia progression is specified by a double exponential growth function. Optom Vis Sci 2005;82(4):286-97. doi: 10.1097/01.opx.0000159370.66540.34 [published Online First: 2005/04/15]
- Goss DA, Winkler RL. Progression of myopia in youth: age of cessation. Am J Optom Physiol Opt 1983;60(8):651-8. doi: 10.1097/00006324-198308000-00002 [published Online First: 1983/08/01]











