
July 1, 2020
By Koumbo Ornella
PhD candidate, Brien Holden Vision Institute
 Emmetropisation is a process by which the components of the eye change/develop to achieve the ideal refractive state where vision is optimal for far objects.1 In human newborns, the refractive state of the eye is that of hyperopia of approximately +2.00D; this hyperopia reduces in magnitude over time until the eye becomes emmetropic. It is said that eye growth is rapid in the initial years, with the eye achieving 90 percent of adult proportions by the age of 3-4 years; after that, the growth decelerates and continues at a slower pace until around 6-8 years.2 The changes in eye growth involve all the major determinants of refractive power, including corneal curvature3, axial length4, and the crystalline lens5 (see Figure 1).
Emmetropisation is a process by which the components of the eye change/develop to achieve the ideal refractive state where vision is optimal for far objects.1 In human newborns, the refractive state of the eye is that of hyperopia of approximately +2.00D; this hyperopia reduces in magnitude over time until the eye becomes emmetropic. It is said that eye growth is rapid in the initial years, with the eye achieving 90 percent of adult proportions by the age of 3-4 years; after that, the growth decelerates and continues at a slower pace until around 6-8 years.2 The changes in eye growth involve all the major determinants of refractive power, including corneal curvature3, axial length4, and the crystalline lens5 (see Figure 1).
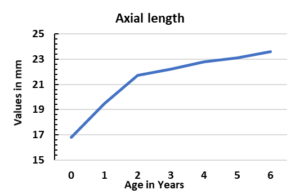
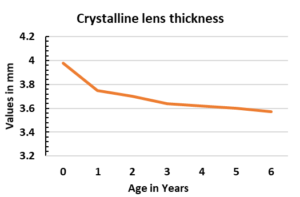
Figure 1:
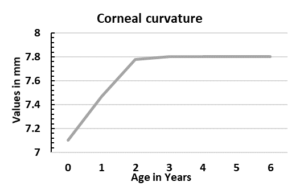
The cornea averages 49.00D at birth and loses refractive power with age as a result of the cornea flattening.6 The radius of curvature of the cornea changes approximately from 7.1 mm to 7.7 mm in the first year of life and 0.1 mm in the second year before reaching adult eye dimensions.
With respect to axial length, the length of a newborn is 16.8 mm and is found to increase by approximately 3.9 mm in the first two years of life, then 1.2 mm between the second and the fifth year, reaching 23.6 mm in the early adult years.4,7
At the same time, the crystalline lens also loses power with lengthening radii of curvature till adult years.5,8 The thickness of the crystalline lens at birth averages 3.9 mm and reduces over time as well. Also, an increase in anterior chamber depth/vitreous chamber depth is observed.
It has been said that emmetropisation is the result of both passive and active processes.9,10 The passive process is attributed to physical and genetic determinants modulating eye growth. The active process is regulated by the retinal image and feedback mechanisms and, consequently, an adjustment of the axial length. In passive emmetropisation, there is considered to be a proportional enlargement of the eye and the active emmetropisation a fine-tuning process that complements passive emmetropisation.9 Ametropia results when the changes are not proportional or a result of heredity, geographical, and environmental influences.11
Given that the cornea appears to play little or no role in the process of emmetropisation after infancy and early childhood, the main ocular components responsible for differences in the emmetropisation process are thought to be the axial length and the crystalline lens.
It is known that there are some racial and ethnic anatomical differences in the ocular structures. Between Asian and Caucasian/white children’s eyes, Asians eyes have smaller anterior segments (corneal diameter, corneal curvature, and anterior chamber width) than Caucasian eyes.12,13 There have not been many studies that have directly compared emmetropisation in Asian and Caucasian eyes. A multi-ethnic study conducted in 2013 in children aged 6-72 months revealed that myopia was relatively more prevalent among Asian children compared to Non-Hispanic white children.14 Also, hyperopia was the most common refractive error in both Asian and Non-Hispanic white children.14 This indicates that there may be differences in the active and passive mechanisms, or as has been suggested for myopic refractive errors, there may be significant environmental influences at play. Irrespective of the mechanism, it may be that an Asian eye will demonstrate more rapid growth than, for example, a Hispanic eye.
So how to determine if ocular growth is normal or not? Monitoring refractive error and axial length change may indicate if a child is progressing faster than age indicated norms. In this regard, measurements of axial length with interferometry are more accurate, as indicated by repeatability measurements (axial length change 0.12 µm versus subjective refraction ±0.50D). In this regard, it appears that there now seems to be some data for age-dependent normative data/percentiles curves for axial length.15,16,17 Comprehensive percentile curves are yet to be available, but a summary of specific percentiles is provided in Table 1 published at https://reviewofmm.com/the-gold-standard-monitoring-myopia-progression-via-measuring-axial-length/. Such percentile curves serve to indicate if eye growth is rapid or excessive, may indicate future risk of onset or progression of myopia (depending on the baseline refractive error state), and may aid clinicians with an appropriate management strategy.

Koumbo Ornella, PhD candidate, Brien Holden Vision Institute
- Wildsoet C. Active Emmetropization—Evidence for Its Existence and Ramifications for Clinical Practice. Ophthalmic and Physiological Optics 1997;17:279-90.
- Hammond CJ. Emmetropization, Refraction and Refractive Errors: Control of Postnatal Eye Growth, Current and Developing Treatments. Pediatric Ophthalmology and Strabismus, Expert Consult-Online and Print, 4: Pediatric Ophthalmology and Strabismus 2012:31.
- Inagaki Y. The Rapid Change of Corneal Curvature in the Neonatal Period and Infancy. Archives of Ophthalmology 1986;104:1026-7.
- Fledelius HC, Christensen AC. Reappraisal of the Human Ocular Growth Curve in Fetal Life, Infancy, and Early Childhood. British Journal of Ophthalmology 1996;80:918-21.
- Iribarren R. Crystalline Lens and Refractive Development. Progress in retinal and eye research 2015;47:86-106.
- EHLERS N, SØRENSEN T, BRAMSEN T, POULSEN EH. Central Corneal Thickness in Newborns and Children. Acta ophthalmologica 1976;54:285-90.
- LARSEN JS. The Sagittal Growth of the Eye: Iv. Ultrasonic Measurement of the Axial Length of the Eye from Birth to Puberty. Acta ophthalmologica 1971;49:873-86.
- Wood IC, Mutti DO, Zadnik K. Crystalline Lens Parameters in Infancy. Ophthalmic and Physiological Optics 1996;16:310-7.
- Brown NP, Koretz JF, Bron AJ. The Development and Maintenance of Emmetropia. Eye 1999;13:83-92.
- Yackle K, Fitzgerald D. Emmetropization: An Overview. J Behav Optom 1999;10:38-43.
- Flitcroft D. Emmetropisation and the Aetiology of Refractive Errors. Eye 2014;28:169-79.
- Qin B, Tang M, Li Y, et al. Anterior Segment Dimensions in Asian and Caucasian Eyes Measured by Optical Coherence Tomography. Ophthalmic Surgery, Lasers and Imaging Retina 2012;43:135-42.
- Blake CR, Lai WW, Edward DP. Racial and Ethnic Differences in Ocular Anatomy. International ophthalmology clinics 2003;43:9-25.
- Wen G, Tarczy-Hornoch K, McKean-Cowdin R, et al. Prevalence of Myopia, Hyperopia, and Astigmatism in Non-Hispanic White and Asian Children: Multi-Ethnic Pediatric Eye Disease Study. Ophthalmology 2013;120:2109-16.
- Tideman JWL, Polling JR, Vingerling JR, et al. Axial Length Growth and the Risk of Developing Myopia in European Children. Acta ophthalmologica 2018;96:301-9.
- Sankaridurg P, Naduvilath T, He X, et al. Axial Length and Axial Length/Corneal Curvature Percentiles for Chinese Cohort Aged 4 to 18 Years. Investigative Ophthalmology & Visual Science 2020;61:2689-.
- Diez PS, Yang L-H, Lu M-X, et al. Growth Curves of Myopia-Related Parameters to Clinically Monitor the Refractive Development in Chinese Schoolchildren. Graefe’s Archive for Clinical and Experimental Ophthalmology 2019;257:1045-53.











