
May 15, 2023
By Jeff Anshel, OD, FAAO
High glycemic load carbohydrate diets may alter the genetic influence of the growth of the sclera and choroid, which will induce permanent changes in the development and progression of myopia, particularly during periods of childhood growth.

Within the eye care community, there is consensus that the cause of juvenile-onset myopia involves genetic and environmental elements. The rise in the prevalence of myopia has been too rapid to be explained by genetic factors alone and thus suggests a substantial role of environmental influences. Numerous studies have demonstrated that near point work is related to myopia. However, all people in industrialized countries must do regular near work during childhood education, yet only a certain percentage of the population ultimately develops myopia. Also, the interaction of genetic and environmental components alone to create refractive error remains speculative. Perhaps there is something else. For example, little attention has been paid to the role of nutrition in the development and advancement of myopia . . . until now.
The Evolutionary Perspective
When considering the genetic influence on ocular growth and function, we must first examine our ancestral genetic makeup. Early Homo sapiens lived about 160,000 years ago and are considered to be anatomically modern Homo sapiens.1 We can infer that significant myopia was not likely present in the population since these early humans required clear distance vision to escape predators, find food, and recognize other species members and a host of environmental dangers. Thus, any gene or genes that would produce significant myopia would be lethal and rapidly eliminated by natural selection.
Dietary-Induced Hyperinsulinemia and Myopia
The diets of hunter-gatherer civilizations are typically considered high protein with moderate levels of fat and low levels of carbohydrate when compared to modern Western diets.2 Additionally, the carbohydrates present in hunter-gatherer diets were typically of a low glycemic index. They are slowly absorbed and produce a gradual and minimal rise in blood glucose and insulin levels compared to the sugars and refined starches in modern western diets.3
The glycemic index ranks carbohydrates on a scale from 0 to 100 according to the extent to which they raise blood sugar levels after eating. High glycemic index foods are rapidly digested and absorbed and result in marked fluctuations in blood sugar levels. Low glycemic index foods, by virtue of their slow digestion and absorption, produce gradual rises in blood sugar and insulin levels, and have proven benefits for health. The glycemic index is a measure influenced by the particle size, processing technique, and relative fiber, protein, and fat content of a carbohydrate food. A glycemic index of over 70 is considered high, 55-70 is medium, and lower than 55 is low. A review of this rating system can be found at: www.glycemicindex.com (Figure 1)
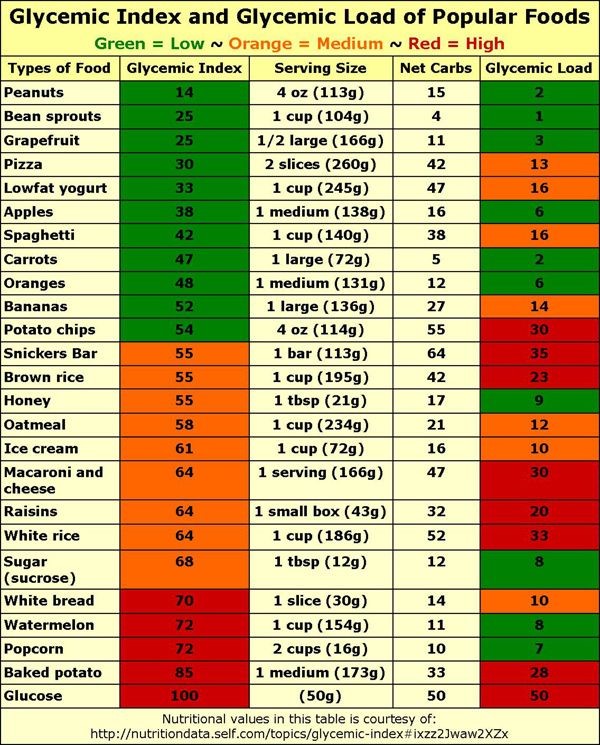
Figure 1: The glycemic index ranks carbohydrates on a scale from 0 to 100 according to the extent to which they raise blood sugar levels after eating.
The glycemic load, a function of the net carbohydrate intake and its glycemic index, estimates how much a food raises a person’s blood glucose level following its consumption. It is calculated by taking each food’s glycemic index x carb content/100. For example, a high glycemic food such as watermelon (index = 72) only contains 11 net carbohydrates and thus has a glycemic load of only 8, whereas white rice (index = 64) contains 52 net carbohydrates and has a glycemic load of 33. A glycemic load of 20 or higher is considered high.3
The average glycemic load of foods in industrialized countries has continually increased, primarily from consuming refined cereals and sugars.4 Populations in more rural areas of industrialized and non-industrialized countries typically have limited access to these processed foods, sugars, and refined cereal products.5 Accordingly, their diets are usually comprised of locally grown, minimally processed foods, and hence the glycemic load of these traditional foods is generally lower than highly processed and packaged food.
Over the past 30+ years, evidence has shown that consuming a westernized diet promotes the development of both acute and chronic hyperinsulinemia, which has also been termed “pre-diabetes.” Numerous studies have demonstrated that the addition of sucrose in the diet of both normal and hyperinsulinemia subjects causes an increase in post-prandial insulin levels.6-8 There is evidence that insulin has direct ocular growth-promoting and indirect effects via the induction of insulin-like growth factors, leading to decreased insulin-like growth factor binding protein (IGFBP), also implicated in ocular growth.9
Collectively, these studies6-9 show that increasing consumption of high levels of refined carbohydrates, especially those considered high caloric foods, is particularly responsible for the worsening of glycemic control and, therefore, insulin resistance and compensatory hyperinsulinemia. It is this state of hyperinsulinemia that can lead to continued growth of the sclera.
Hyperinsulinemia and Insulin-Like Growth Factor (IGF) and IGF Binding Proteins
The metabolic reactions accompanying hyperinsulinemia are complex and have profound effects on growth and development, including within the eye. The pancreas produces post-prandial levels of insulin, while the liver secretes insulin-like growth factor-1 (IGF-1) as well as the IGFBP-1, which controls the action of IGF-1. Hyperinsulinemia suppresses the secretion of IGFBP-1 from the liver, which in turn increases free IGF-1 in the serum.10 Increased circulating levels of free IGF-1 is a potent stimulator of growth in all tissues. (Figure 2)
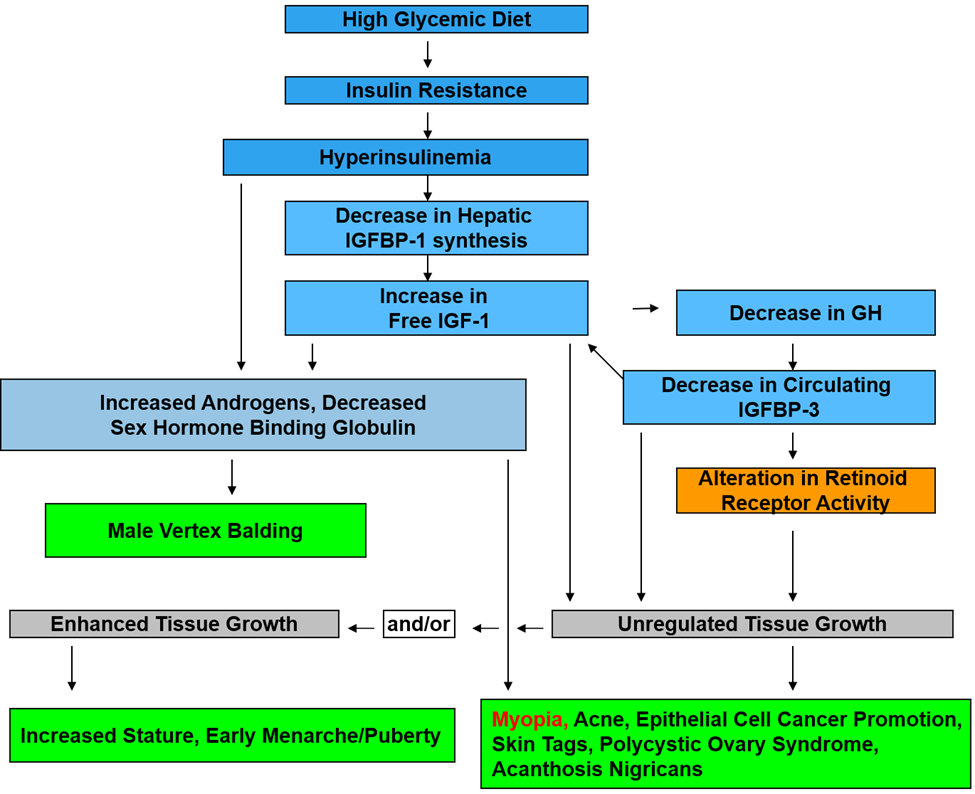
Figure 2
Retinoic Acid Receptors and Hyperinsulinemia
Retinoic acid, which is required for growth and development, is a metabolite of vitamin A that mediates the functions of the vitamin. The all-trans-retinoic acid (ATRA) form is essential in the growth of higher animals. During early embryonic development, ATRA helps determine the orientation of the posterior portion of the embryo. In the sclera, ATRA inhibits glycosaminoglycan synthesis, thereby thinning the sclera and promoting axial elongation.11
Additional Nutrients that Affect Myopia Development
Many nutrients are required for proper growth and development. A balance of 13 essential vitamins and 15 essential minerals is critical for proper utilization. Some of these nutrients have been associated with the development of myopia, specifically vitamin A (as discussed above), as well as vitamin B2, and vitamin C.
Vitamin B2 (riboflavin) is involved in energy metabolism, cell respiration, antibody production, growth, and development. It is essential for the metabolism of carbohydrates, protein, and fats. Additionally, riboflavin is involved in the metabolism of niacin, vitamin B6, and folate.
Riboflavin is used in the recently established collagen crosslinking, which is an effective method for halting the progression of keratectasia in patients with keratoconus. UVA light forms new bonds between the collagen fibers in the cornea, making them stronger. Given this effect of UVA on collagen, one could postulate an internal interaction of riboflavin and UVA radiation with time spent outdoors. One study showed that oral administration of riboflavin with whole body UVA irradiation could increase the strength and stiffness of the sclera by altering biochemical and biomechanical properties.
Another study showed that violet light (VL, 360-400 nm wavelength) suppresses myopia progression, with violet-light-transmitting contact lenses suppressing myopia progression the most. The results suggested that violet light is one of the critical outdoor environmental factors for myopia control. Since violet light is apt to be excluded from our modern society due to universal UV protection, violet light exposure can be a preventive strategy against myopia progression.12
Vitamin C is essential for collagen production in the body by serving as a co-factor for two enzymes responsible for stabilizing collagen molecules. Vitamin C deficiency leads to impaired collagen synthesis. Vitamin C is water soluble and flushes out of the body in two to three hours, so a single daily dose is not very effective.
Does Insulin Resistance Influence Myopia?
Given the unprecedented rise in myopia among people of East Asian descent, it is vital to review trends in their dietary habits. It is documented that this demographic tends to be more insulin resistant than people of European descent.13,14 Reviewing the demographics of diabetes worldwide, it should be noted that over half of the world’s population with diabetes is centered in Western Pacific and Southeast Asian regions. (Figure 3) The higher rates of myopia in East Asian populations may, in part, be due to their increased genetic susceptibility to insulin resistance. It is important to note that white rice, which has a glycemic load of 33 (remember, anything over 20 is considered high), is a staple of the diet in Asia.
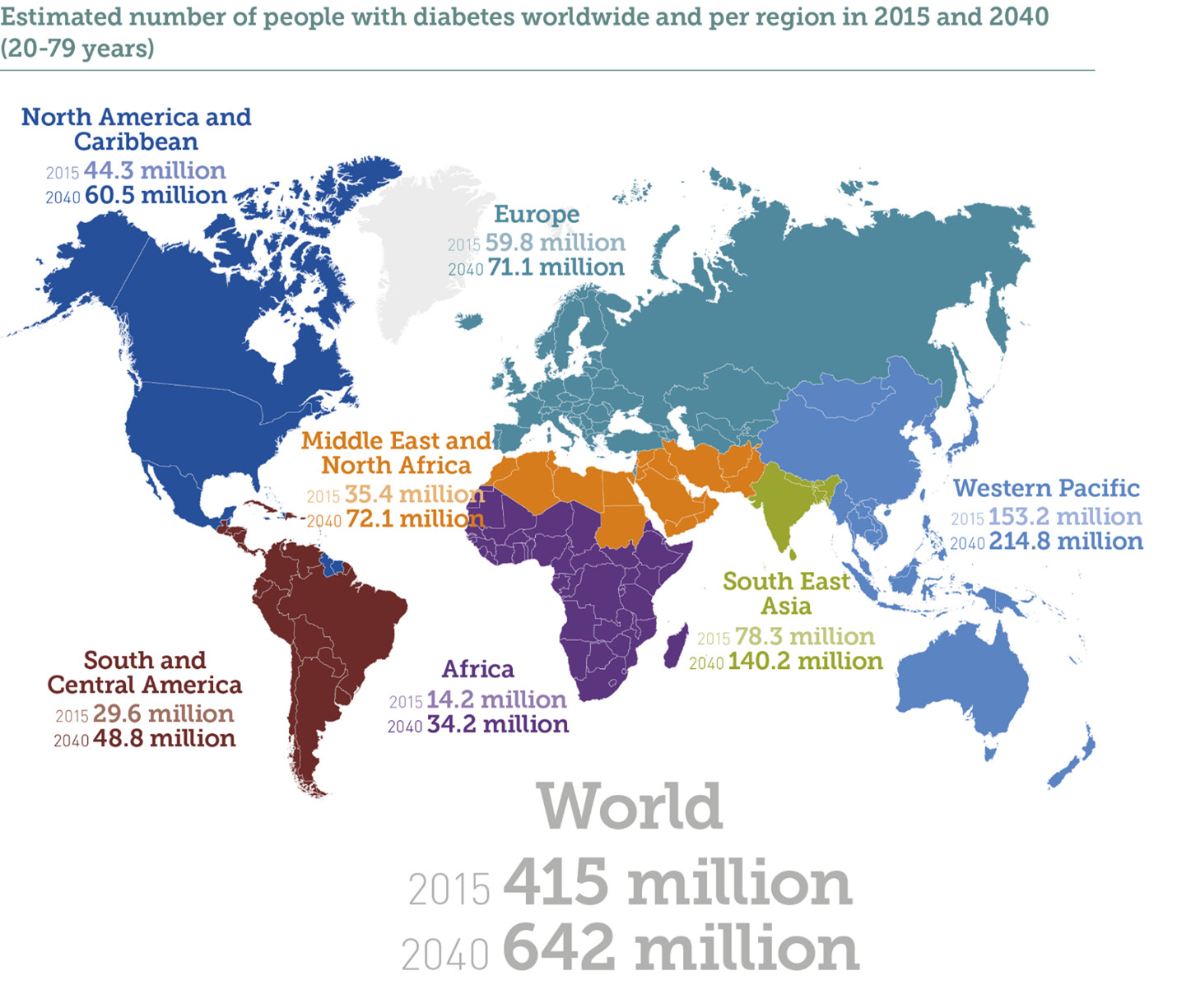
Figure 3: The estimated number of people with diabetes worldwide and per region in 2015 and 2040.
It is possible that the etiology of juvenile-onset myopia does not have a single cause but might result from a “perfect storm” of several factors. It has been established that newborns typically exhibit low hyperopia.15 When taking in a westernized diet that includes highly refined grains and carbohydrates, they could tend toward the development of hyperinsulinemia. The growth pattern of the sclera thins and continues to elongate due to the excessive carbohydrate influences, combined with a lack of outdoor lighting and an increase of near point tasks (especially the digital display variety). This depleted nutrition pattern might continue with a vitamin B2 deficiency and intraocular pressure increases with excessive accommodation leading to continued scleral elongation and subsequent myopia. Real world human studies would be required to confirm how these interactions might lead to the current state of myopia development.
In conclusion, a review of the above-referenced studies suggests that high glycemic load carbohydrate diets may alter the genetic influence of the growth of the sclera and choroid, which will induce permanent changes in the development and progression of myopia, particularly during periods of childhood growth.
 |
Dr. Jeffrey Anshel is a 1975 graduate of the Illinois College of Optometry. He has written numerous articles and ten books regarding nutritional influences on vision and computer vision concerns. Dr. Anshel is the principal of Corporate Vision Consulting, where he addresses nutrition and eye health, as well as digital eyestrain. He lectures internationally to ergonomic professionals and eye care providers on vision health topics. Dr. Anshel is a Fellow of the American Academy of Optometry and the Founder and Past President of the Ocular Wellness and Nutrition Society. He maintains a consulting practice in Kapaa, Hawaii. |
References
- White, Tim D.; Asfaw, Berhane; Degusta, David; et al. “Pleistocene Homo sapiens from Middle Awash, Ethiopia“. Nature. 2003;423 (6941):742–7.
- www.glycemicindex.com accessed 4/1/2023.
- Cordain L. Cereal grains: humanity’s double-edged sword. World Rev Nutr Diet 1999;84: 19–73.
- Thorburn AW, Brand JC & Truswell AS. Slowly digested and absorbed carbohydrate in traditional bushfoods. a protective factor against diabetes? Am J Clin Nutr 1987;45:98–106.
- Cleave TL. The Saccharine Disease. John Wright & Sons Ltd. Bristol, UK. 1974;6–27.
- Trowell H. Dietary Fibre, Fibre-Depleted Foods and Disease. In: Trowell H, Burkitt D, Heaton K & Doll R (eds.). Academic Press. 1985 New York, USA.1–20.
- Reiser S, Handler HB, Gardner LB, et al. Isocaloric exchange of dietary starch and sucrose in humans. II. Effect on fasting blood insulin, glucose, and glucagon and on insulin and glucose response to a sucrose load. Am J Clin Nutr 1979;32:2206–16.
- Coulston AM, Liu GC & Reaven GM. Plasma glucose, insulin and lipid responses to high-carbohydrate low-fat diets in normal humans. Metabolism 1983;32:52–56.
- Reiser S, Bohn E, Hallfrisch J, et al. Serum insulin and glucose in hyperinsulinaemic subjects fed three different levels of sucrose. AmJ Clin Nutr 1981;34:2348–58.
- Galvis, V, et al. “Is myopia another clinical manifestation of insulin resistance?” Medical Hypotheses 2016;90:32-40.
- Metlapally, R., Ki, C.S., Li, Y. et al. Genetic association of insulin-like growth factor-1 polymorphisms with high-grade myopia in an international family cohort. IOVS 2010;51(9),4476-79.
- Li X, Wu M, Zhang L, et al. Riboflavin and ultraviolet A irradiation for the prevention of progressive myopia in a guinea pig model. Exp Eye Res 2017;165:1–6.
- Beischer NA, Oats JN, Henry OA, et al. Incidence and severity of gestational diabetes mellitus according to country of birth in women living in Australia. Diabetes 1991;40:35–8.
- King H & Rewers M. Global estimates for prevalence of diabetes mellitus and impaired glucose tolerance in adults. WHO Ad Hoc Diabetes Reporting Group. Diabetes Care 1993;16:157–77.
- Morgan IG, Rose KA, Ellwein LB; Refractive Error Study in Children Survey Group. Is emmetropia the natural endpoint for human refractive development? An analysis of population-based data from the refractive error study in children (RESC). Acta Ophthalmol. 2010;88(8):877-84.











