
July 2, 2019
By Cathleen Fedtke, Dipl. Ing. (FH), PhD, FAAO
Senior Research Fellow, Project Manager – Brien Holden Vision Institute
The use of the spectacle lenses for myopia management dates back more than 30 years ago, when bifocal spectacle lenses prescribed to children with near-esophoria showed a reduction in myopia progression.1, 2 Since then, several spectacle lens-based approaches have been assessed based on the two main theories of myopia development and progression: the Accommodative Lag and the Peripheral Hyperopic Defocus theory.
While the Accommodative Lag theory presumes that an insufficient amount of accommodation during near work – as reported in myopic children – causes retinal blur. The Peripheral Hyperopic Defocus theory is based on the findings that in myopic eyes, peripheral refraction profiles are relatively hyperopic; hence, it was hypothesised that both kinds of hyperopic blur signals could be a trigger for eye growth.
Optical intervention methods for both theories therefore aim to reduce hyperopic defocus, either centrally during near work or in the peripheral visual field. The treatment modalities with spectacle lenses include under-correction with single vision spectacle lenses,3-6 reduction of accommodative lag and/or reduction of peripheral hyperopic defocus (at least in the inferior visual field) with progressive addition spectacle lenses (PALs),7-12 positively aspherized progressive addition lenses13 or with executive bifocal or executive prismatic bifocal spectacles.14 More recently, peripherally modified single vision spectacle lenses, such as peripheral defocus-correcting spectacle lenses15 and Defocus Incorporated Multiple Segments (DIMS) spectacle lenses, have also been shown to significantly reduce myopia progression.16
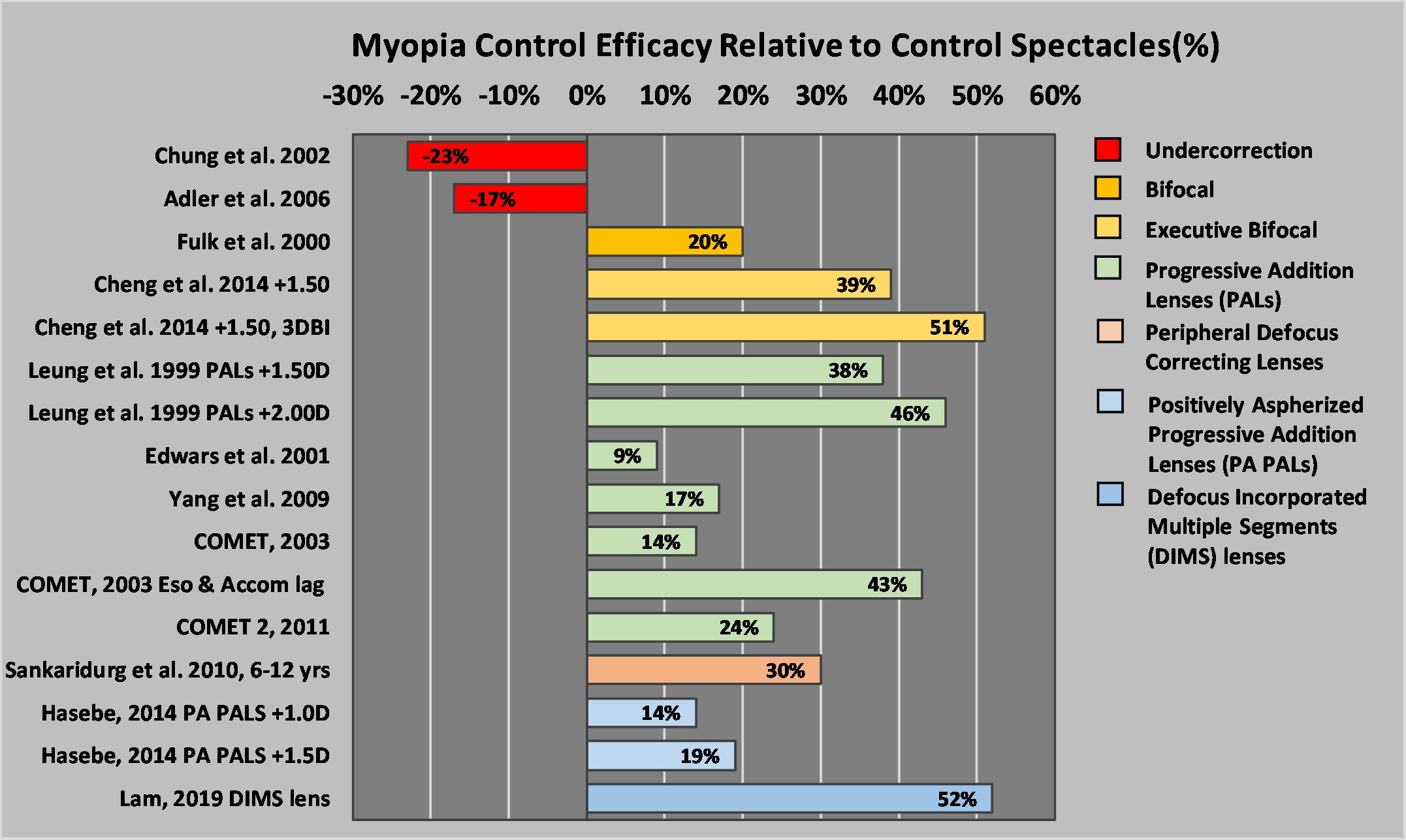 Using under-correction to reduce the accommodative demand during near work has been shown to be an ineffective optical intervention to slow the progression of myopia. Whilst some studies showed no difference between under-corrected and fully corrected children,3, 6 the studies by Chung et. al.5 and Adler et. al.4 reported significantly higher rates of myopia progression in the under-corrected group. Based on this, there is no support that this strategy should be used to control myopia progression.
Using under-correction to reduce the accommodative demand during near work has been shown to be an ineffective optical intervention to slow the progression of myopia. Whilst some studies showed no difference between under-corrected and fully corrected children,3, 6 the studies by Chung et. al.5 and Adler et. al.4 reported significantly higher rates of myopia progression in the under-corrected group. Based on this, there is no support that this strategy should be used to control myopia progression.
Although traditional bifocal lenses and PALs are the most commonly accessible and, hence, most studied spectacle lens-based interventions, such lenses have shown a relatively low efficacy in slowing myopia progression. Their treatment effect, however, improved in children with esophoria at near and/or when children had accommodative lags.11
Of the seven different spectacle lens-based, myopia-control modalities, the greatest efficacy was reported with the recent DIMS lens, with reduction in myopia progression and axial elongation of 52 percent and 62 percent, respectively.16 The DIMS lens features a clear central zone (9 mm diameter) surrounded by an array of multiple defocus segments (each 1.03 mm in diameter and a power of +3.50D), which are arranged in a hexagonal pattern covering a visual field of about 40 degrees. Unlike most of the other traditional spectacle lens-based approaches that provide extra plus during near work, the DIMS lens is entirely based on the hypothesis that imposing myopic defocus in the peripheral visual field, during distance and near viewing, can inhibit ocular growth. Due to its small central zone, this lens must be well fitted to provide good visual performance.
A similar myopia control efficacy of 51 percent was achieved with executive prismatic bifocal spectacle lenses (i.e. +1.50D add power and 3-Δ-near base-in prism) in children with high rates of myopia progression (i.e. ≥ 0.50 D in the preceding year) and lower lags of accommodation.14 The efficacy was reduced to 39.3 percent for the second test group, who wore executive bifocal spectacle lenses without the near prisms. However, the change in axial length was similar between both groups (i.e. Δ bifocals 34.1 percent versus bifocals 30.5 percent). Since this study tested executive bifocal lenses in already progressing children, care needs to be taken when comparing these results to other studies. In terms of lens design differences, it may be speculated that a better efficacy reported with executive bifocal lenses may be due to the significantly larger near portion, which during distance viewing would provide a greater amount of peripheral myopic defocus in the inferior visual field than with PALs or other traditional bifocal lenses, e.g. flat-top (D-segment).
Besides the spectacle lens strategies based on the Accommodative Lag and Peripheral Hyperopic Defocus theories, a relatively new strategy is based on incorporation of light-diffusion technology in spectacle lenses. While reports of early stage clinical trials are said to be promising (no published data yet), a large, multi-centre, randomised clinical trial is currently underway to assess this new technology in terms of safety and efficacy.17
Overall, spectacle lenses are a practical, generally well-accepted and safe method to correct refractive errors in children. For children whose onset is at an earlier age, where other modalities such as contact lenses are not really suitable (i.e. < 7-8 years of age), myopia control spectacle lenses should be considered as the first strategy. Younger children are prone to greater annual progression and are likely to achieve higher levels of myopia; therefore, to ensure maximum benefit, early intervention is critical. Further, to ensure that the best treatment effect and visual performance can be achieved, it is important that such spectacle lenses are well fit and regularly monitored. Depending on the risk factors and the rate of progression, additional intervention strategies, such as pharmaceutical (e.g. atropine) and/or environmental interventions (less near work, spending more time outdoors), may be considered in combination with myopia-control spectacle lenses. When appropriate, other optical interventions that have shown good efficacy in slowing myopia progression (e.g. multifocal or orthokeratology contact lenses) may also be considered.
References:
- Goss DA. Effect of bifocal lenses on the rate of childhood myopia progression. Am J Optom Physiol Opt. 1986;63(2):135-41.
- Fulk GW, Cyert LA, Parker DE. A randomized trial of the effect of single-vision vs. bifocal lenses on myopia progression in children with esophoria. Optom Vis Sci. 2000;77(8):395-401.
- Li SY, Li SM, Zhou YH, et al. Effect of undercorrection on myopia progression in 12-year-old children. Graefes Arch Clin Exp Ophthalmol. 2015;253(8):1363-8.
- Adler D, Millodot M. The possible effect of undercorrection on myopic progression in children. Clin Exp Optom. 2006;89(5):315-21.
- Chung K, Mohidin N, O’Leary DJ. Undercorrection of myopia enhances rather than inhibits myopia progression. Vision Res. 2002;42(22):2555-9.
- Koomson NY, Amedo AO, Opoku-Baah C, et al. Relationship between Reduced Accommodative Lag and Myopia Progression. Optom Vis Sci. 2016;93(7):683-91.
- Leung JT, Brown B. Progression of myopia in Hong Kong Chinese schoolchildren is slowed by wearing progressive lenses. Optom Vis Sci. 1999;76(6):346-54.
- Hasebe S, Ohtsuki H, Nonaka T, et al. Effect of progressive addition lenses on myopia progression in Japanese children: a prospective, randomized, double-masked, crossover trial. Invest Ophthalmol Vis Sci. 2008;49(7):2781-9.
- Gwiazda J, Hyman L, Hussein M, et al. A randomized clinical trial of progressive addition lenses versus single vision lenses on the progression of myopia in children. Invest Ophthalmol Vis Sci. 2003;44(4):1492-500.
- Yang Z, Lan W, Ge J, et al. The effectiveness of progressive addition lenses on the progression of myopia in Chinese children. Ophthalmic Physiol Opt. 2009;29(1):41-8.
- Correction of Myopia Evaluation Trial 2 Study Group for the Pediatric Eye Disease Investigator G. Progressive-addition lenses versus single-vision lenses for slowing progression of myopia in children with high accommodative lag and near esophoria. Invest Ophthalmol Vis Sci. 2011;52(5):2749-57.
- Berntsen DA, Sinnott LT, Mutti DO, Zadnik K. A randomized trial using progressive addition lenses to evaluate theories of myopia progression in children with a high lag of accommodation. Invest Ophthalmol Vis Sci. 2012;53(2):640-9.
- Hasebe S, Jun J, Varnas SR. Myopia control with positively aspherized progressive addition lenses: a 2-year, multicenter, randomized, controlled trial. Invest Ophthalmol Vis Sci. 2014;55(11):7177-88.
- Cheng D, Woo GC, Drobe B, Schmid KL. Effect of bifocal and prismatic bifocal spectacles on myopia progression in children: three-year results of a randomized clinical trial. JAMA Ophthalmol. 2014;132(3):258-64.
- Sankaridurg P, Donovan L, Varnas S, et al. Spectacle lenses designed to reduce progression of myopia: 12-month results. Optom Vis Sci. 2010;87(9):631-41.
- Lam CSY, Tang WC, Tse DY, et al. Defocus Incorporated Multiple Segments (DIMS) spectacle lenses slow myopia progression: A 2-year randomised clinical trial. Br J Ophthalmol. 2019.
- Available from https://clinicaltrials.gov/ct2/show/NCT03623074

Cathleen Fedtke, Dipl. Ing. (FH), PhD, FAAO, is a Senior Research Fellow, Project Manager at the Brien Holden Vision Institute











