
April 1, 2021
By Huy Tran, MD, and Padmaja Sankaridurg, PhD
“Should a combination strategy be routinely presented as an option for myopia control? There are several considerations other than efficacy alone.”

Of the various myopia management approaches, single vision spectacle and contact lenses simply correct the vision impairment. In contrast, atropine at various concentrations slows myopia but does not correct for vision impairment. Myopia control optical devices such as spectacles (including progressive addition, peripheral defocus management, executive bifocals, and multiple segment lenses), soft contact lenses (multifocal like and extended depth of focus contact lenses), and orthokeratology (OrthoK) not only correct but also reduce the risk of progression to a varying extent.
Combination therapy is a logical and methodical approach to improve either the patient experience and/or efficacy obtained with monotherapy alone. Indeed, the approach of improving patient experience is well-known and applied frequently. For example, children prescribed higher concentrations of atropine are prescribed bifocal or multifocal spectacle lenses to restore vision for both distance and near[1-3]. However, of greater interest is the aim of improving efficacy over that realized with monotherapy alone. Many precedents exist for this approach in managing health and disease, where combination therapies are frequently used to boost efficacy. They are particularly useful where multiple pathways are involved in the condition as it allows targeting via more than a single pathway. It is probable that some practitioners already adopt this route using the available evidence on efficacy and risks versus benefits to maximize efficacy for their myopic patients. An example would be recommending increased outdoor time in combination with an optical intervention.
Combination Options Assessed in Clinical Trials
Thus far, efforts have been directed to determine if the efficacy realized with optical devices can be improved further when used in combination with atropine.
Atropine plus OrthoK: Four trials (both retrospective and prospective) evaluated dual therapy (atropine plus OrthoK), and all found an improved efficacy compared to monotherapy (OrthoK alone)[4-7]. In a retrospective study, eyes were categorized as <-6.00D and ≥-6.00D and further sub-grouped to receive dual therapy (with 0.125% or 0.025% atropine) or monotherapy. Dual therapy demonstrated slower progression compared to monotherapy for most but not all of the subgroups[4]. In a prospective trial, following three months of OrthoK, children were randomized to monotherapy or dual therapy (0.01% atropine at night). At the end of the year, dual therapy resulted in a significantly slower change in axial length.[6] Similar results were obtained in a two-year randomized trial.[5] In a separate retrospective study, in Year 1, all participants received OrthoK, whereas, in Year 2, 0.01% atropine was added for those with axial length change >0.25mm. Axial elongation significantly reduced in Year 2 with dual therapy compared to a historical control group with fast progression.[7] Figure 1 illustrates the percentage change in control obtained with combination therapy compared to monotherapy.
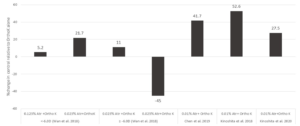
Figure 1: Percent change in control with combination therapy relative to orthokeratology alone
Atropine plus bifocal/multifocal contact lenses or spectacles: Evidence is sparse for the use of atropine in combination with contact lenses or spectacles. The bifocal and atropine study aims to determine if the use of 0.01% atropine in conjunction with a center-distance soft bifocal contact lens (+2.50D Add) provides better efficacy compared to the soft bifocal lens alone. The results of this three-year trial are yet to be published.[8] In a randomized clinical trial spanning 18 months, the mean progression of children randomized to atropine 0.5% plus multifocal spectacles progressed much slower compared to either multifocal lenses alone or single-vision spectacles. [9]
It should be noted that none of the aforementioned clinical trials evaluated the efficacy with atropine alone to determine if the efficacy with dual therapy was greater than that of atropine alone. A single report compared efficacy data with dual therapy to other atropine data and concluded that dual therapy performed better.[5] The mechanisms underlying the improved efficacy with dual therapy remain unclear; hypotheses include: a) larger pupil resulting from atropine use promoting myopic defocus from OrthoK, b) the blocking of muscarinic receptors aids in achieving myopia control via a different pathway, and c) the larger pupil size may have improved violet light exposure.[6]
Further support for combination treatments involving defocus and atropine is from a study where 0.3% atropine was found to increase choroidal thickness by approximately 20 µm and consistently over a six-month period. While additional short periods of myopic defocus resulted in a further increase in choroidal thickness, no such change or thinning was observed with hyperopic defocus. It was considered that defocus and atropine might be operating through two different mechanisms resulting in increased choroidal thickness[10]. However, in another study homatropine similarly blocked the thinning effect with hyperopic defocus, but no additive effect was found when used in combination with myopic defocus[11].
Prescribing Combination Therapies in Practice
Although further work is needed to understand the underlying mechanisms and optimization of treatment methods, the results from studies so far are encouraging for combination treatments. Should then a combination strategy be routinely presented as an option for myopia control? There are several considerations other than efficacy alone. Since combination therapy involves two or more systems, it involves additional effort for both practitioner and patient as well as additional costs. Combination therapy may also result in additional side effects, such as larger pupils, and may also promote non-compliance.
Furthermore, suppose combination therapy is instituted as a first-line treatment before monotherapy and does not produce the intended benefits. In that case, it may be challenging to know which of the two therapies is not effective. On the other hand, combination therapy provides a greater chance of efficacy. It may be a valuable option, especially in children at risk of fast progression, where the risk of side effects and rebound of atropine precludes the use of higher doses of atropine. And it also provides a means to improve efficacy in those who may not be appropriately responding to monotherapy alone.

Huy Tran, MD, is a pediatric ophthalmologist with the Myopia Control Clinic, Hai Yen Eye Care in Ho Chi Minh City, Vietnam, and a PhD candidate at the Brien Holden Vision Institute.

Padmaja Sankaridurg B.Opt, MIP, PhD, is the program Leader, Myopia and Manager, Intellectual Property at the Brien Holden Vision Institute in Sydney, Australia. She is also Conjoint Professor at the School of Optometry and Vision Science, University of New South Wales.
- Syniuta, L. and S. Isenberg, Atropine and bifocals can slow the progression of myopia in children. Binocular vision & strabismus quarterly, 2001. 16(3): p. 203-208.
- CHOU, A.-C., et al., The effectiveness of 0.5% atropine in controlling high myopia in children. 1997. 13(1): p. 61-67.
- Polling, J.R., et al., Effectiveness study of atropine for progressive myopia in Europeans. Eye (Lond), 2016. 30(7): p. 998-1004.
- Wan, L., et al., The Synergistic Effects of Orthokeratology and Atropine in Slowing the Progression of Myopia. J Clin Med, 2018. 7(9).
- Kinoshita, N., et al., Efficacy of combined orthokeratology and 0.01% atropine solution for slowing axial elongation in children with myopia: a 2-year randomised trial. Scientific Reports, 2020. 10(1): p. 1-11.
- Kinoshita, N., et al., Additive effects of orthokeratology and atropine 0.01% ophthalmic solution in slowing axial elongation in children with myopia: first year results. Jpn J Ophthalmol, 2018. 62(5): p. 544-553.
- Chen, Z., et al., Adjunctive effect of orthokeratology and low dose atropine on axial elongation in fast-progressing myopic children-A preliminary retrospective study. Cont Lens Anterior Eye, 2019. 42(4): p. 439-442.
- Huang, J., et al., Bifocal & Atropine in Myopia Study: Baseline Data and Methods. Optom Vis Sci, 2019. 96(5): p. 335-344.
- Shih, Y.F., et al., An intervention trial on efficacy of atropine and multifocal glasses in controlling myopic progression. Acta Ophthalmol Scand, 2001. 79(3): p. 233-6.
- Chiang, S.T.H., P.R.K. Turnbull, and J.R. Phillips, Additive effect of atropine eye drops and short-term retinal defocus on choroidal thickness in children with myopia. Scientific reports, 2020. 10(1): p. 18310-18310.
- Sander, B.P., M.J. Collins, and S.A. Read, The interaction between homatropine and optical blur on choroidal thickness. Ophthalmic Physiol Opt, 2018. 38(3): p. 257-265.











