
June 11, 2020
By Dwight Akerman, OD, MBA, FAAO
Chief Medical Editor, Review of Myopia Management
Myopia is a refractive condition caused by excessive axial length elongation.1 Once considered a simple refractive error with few, if any, long-term eye health consequences, myopia has now been shown to increase the risk of serious, sight-threatening complications, including myopic macular degeneration, retinal detachment, primary open-angle glaucoma, macular hole, retinoschisis, and nuclear & posterior subcapsular cataract.2
Axial length (AL) measurement has not traditionally been considered part of mainstream optometry. The same could have been said for visual field assessment four decades ago and OCT measurements a decade ago. Just as most primary care optometric practices now routinely utilize threshold visual field and OCT instrumentation, it should be the aim of eye care professionals to do the same for AL measurement in pediatric myopia management.
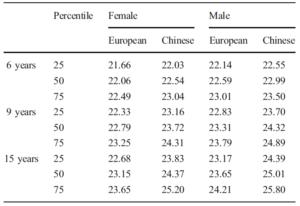
Recently published work has provided insights into typical AL growth rates, enabling the risk of myopia to be assessed, with normative values being published for a cohort of European and Chinese children.3,4 The collected data were reported as percentiles, a term that is well understood for other growth factors such as height and weight. Children below the 50th percentile for AL increase are significantly less likely to become myopic (and almost certainly not be highly myopic), compared to those above the 50th percentile. Children of Chinese ethnicity have longer axial lengths, indicating the higher prevalence of myopia in that population.
Percentiles of AL in 6-, 9-, and 15-year old European and Chinese children of both genders.3,4
High myopia, which is defined as spherical equivalent (SE) of -6.00 D or worse, generally corresponds to AL ≥26 mm, which drastically increases the risk of severe complications later in life. High myopia is currently one of the leading causes of legal blindness in developed countries because of complications occurring in adulthood.5
There are two main options for measuring AL: ultrasound biometry and optical biometry. A-scan ultrasound biometry is not as accurate and a more challenging technique to use on children due to the contact nature of the instrument. There are many options available for optical biometry, covering a range of budget options. Most devices are easy to use on children and are non-invasive.
The main cause of myopia is an increase in axial length. The ocular morbidity increases per mm of axial length, and consists of myopic macular degeneration, retinal detachment, primary open-angle glaucoma, macular hole, retinoschisis, and nuclear & posterior subcapsular cataract.2 AL measurement should be considered the gold standard of myopia management.
Here are details of leading optical biometers for measuring axial length:

IOLMaster 700
IOLMaster 700 Zeiss
The IOLMaster 700 has added a feature called Total Keratonomy (TK) that lets cataract surgeons replace using SWEPT Source OCT. It combines telecentric keratometry measurement of the anterior assumptions about the posterior corneal surface with measurements helping to improve outcomes. Corneal surface with measurement of the posterior corneal surface to calculate Total Keratometry was developed to be compatible with standard formulas and existing IOL constants, allowing surgeons to detect outlier cases.
The device also includes two new Barrett formulas incorporating the new TK value. Features include two new formulas, Barrett TK Universal II and Barrett TK Toric. The device can be used in classic IOL calculation formulas – no need for a second device, third-party software, or an online calculator.

Lenstar LS 900
Lenstar 900 Haag-Streit
The LENSTAR LS 900 does nine measurements in 30 seconds (eight seconds in the United States), including central corneal thickness, lens thickness, pupil diameter, eccentricity of the visual axis, anterior chamber depth, axial length, keratometry, white to white, retinal thickness (N/A in the USA). Axial length is always measured on the central visual axis. It also provides automatic fixation control so that measurements are consistently repeatable.
LENSTAR uses an 820-nanometer superluminescent diode, combined with OLCR technology, which is similar to time-domain OCT. This provides axial length measurements and biometry of the entire eye.

Aladdin HW 3.0
Aladdin HW 3.0 Topcon
The ALADDIN Biometer with corneal topography is intended for biometric determination of axial length, corneal radius, keratometry, corneal thickness, anterior chamber depth, lens thickness, corneal diameter, and pupillometry of the eye. The Aladdin also measures corneal topography. The corneal topography function provides information on changes in the corneal surface.
The Aladdin RX/AL Trend feature allows the operator to monitor and display trends and progression of eye parameters that are related to the onset and evolution of myopia by using the standard measurements performed by the instrument. The data is processed so that it will provide quantitative documentation of axial length changes. Axial length measurements taken with other instruments can be manually incorporated in the Aladdin’s database for reference.
Pentacam AXL
Oculus Pentacam AXL
The Pentacam AXL is a systematic enhancement of the time-tested Pentacam HR technology. In addition to anterior segment tomography, the original function of its predecessor, the Pentacam AXL has integrated axial length measurement, a feature that allows you to make accurate IOL calculations.
References:
1 Meng, W., Butterworth, J., Malecaze, F., & Calvas, P. (2011). Axial length of myopia: a review of current research. Ophthalmologica, 225(3), 127-134.
2 Haarman, A. E., Enthoven, C. A., Tideman, J. W. L., Tedja, M. S., Verhoeven, V. J., & Klaver, C. C. (2020). The Complications of Myopia: A Review and Meta-Analysis. Investigative Ophthalmology & Visual Science, 61(4), 49-49.
3 Tideman, J. W. L., Polling, J. R., Vingerling, J. R., Jaddoe, V. W., Williams, C., Guggenheim, J. A., & Klaver, C. C. (2018). Axial length growth and the risk of developing myopia in European children. Acta ophthalmologica, 96(3), 301-309.
4 Diez, P. S., Yang, L. H., Lu, M. X., Wahl, S., & Ohlendorf, A. (2019). Growth curves of myopia-related parameters to clinically monitor the refractive development in Chinese schoolchildren. Graefe’s Archive for Clinical and Experimental Ophthalmology, 257(5), 1045-1053.
5 Tideman, J. W. L., Snabel, M. C., Tedja, M. S., Van Rijn, G. A., Wong, K. T., Kuijpers, R. W., … & Boon, C. J. (2016). Association of axial length with risk of uncorrectable visual impairment for Europeans with myopia. JAMA ophthalmology, 134(12), 1355-1363.











